



![MESOLIMBIC PATHWAY
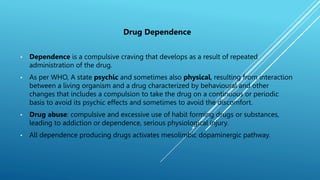
ŌĆó Mesolimbic pathway ( reward pathway) is a dopaminergic
pathway in the brain which connects ventral tegmental area
located in the midbrain to the nucleus accumbens.
ŌĆó The mesolimbic pathway releases dopamine into the nucleus
accumbens and stimulates rewarding system.
ŌĆó Abused drugs [alcohol, opiates, ╬ö9tetrahydrocannabinol (╬ö9-
THC), and psychostimulants, including nicotine] interact with
endogenous neural pathways in the brain.
ŌĆó In particular, they share the common property of activating
mesolimbic dopamine brain reward systems, and virtually all
abused drugs elevate dopamine levels in the nucleus
accumbens.
ŌĆó In nucleus accumbens, ŌłåFosB functions as a master control
protein in the development of drug addiction.
ŌĆó Once it is overexpressed it triggers series of transcription
events that ultimately produce an adaptive state.](https://image.slidesharecdn.com/dependence-240722053302-3f80f5bd/85/Drug-dependence-types-causes-and-mechanism-of-action-7-320.jpg)










Drug dependence types , causes and mechanism of action
- 1. DRUG DEPENDENCE (CELLULAR AND MOLECULAR MECHANISM)
- 2. Drug Dependence ŌĆó Dependence is a compulsive craving that develops as a result of repeated administration of the drug. ŌĆó As per WHO, A state psychic and sometimes also physical, resulting from interaction between a living organism and a drug characterized by behavioural and other changes that includes a compulsion to take the drug on a continuous or periodic basis to avoid its psychic effects and sometimes to avoid the discomfort. ŌĆó Drug abuse: compulsive and excessive use of habit forming drugs or substances, leading to addiction or dependence, serious physiological injury. ŌĆó All dependence producing drugs activates mesolimbic dopaminergic pathway.
- 3. TYPES OF DRUG DEPENDENCE:- 1.Psychic dependence:-A condition in which a drug produces ŌĆó A feeling of satisfaction ŌĆó A Psychic drive that require periodic or continuous administration of the drug. 2.Physical dependence:- Its a state in which ŌĆó A body achieves an adaptive state ŌĆó Causes physical disturbances when the drug is withdrawn. ŌĆó Withdrawal syndrome varies in type and intensity for different classes. 3.Combined dependence:-it involves both psychic and physical dependence terms. ŌĆó An overpowering desire to continue taking the drug in spite of knowing its harmful effects. ŌĆó A tendency to increase the dose. ŌĆó A high tendency to withdrawal syndromes. Drug Dependence Psychic Dependence Combined Dependence Physical Dependence
- 4. Withdrawal Syndrome ŌĆó withdrawal of the psychoactive drugs produces distorted homeostasis leading to the development of a withdrawal syndrome.(discontinuation syndrome). ŌĆó It is a set of symptoms of variable degree of severity which occur on cessation or reduction of psychoactive drugs. ŌĆó A withdrawal syndrome is one of the indicators of a dependence syndrome. ŌĆó Example, the alcohol withdrawal syndrome is characterized by tremor, sweating, anxiety, depression, nausea and malaise.
- 5. DRUGS KNOWN TO CAUSE DEPENDENCE I. Drugs that cause sever psychic and physical dependence: ŌĆó Opiate or morphine type: Morphine and its congeners Codeine, Dihydromorphinone and Heroin, synthetic morphine substituents like Meperidine. ŌĆó Alcohol barbiturate type: Ethyl alcohol, Barbiturates, Paraldehyde, Benzodiazepines and Meprobamate. ŌĆó Nicotine (tobacco) II. Drugs cause definite psychic but mild or questionable physical dependence: ŌĆó Opiate antagonist type: Nalorphine (morphine antagonist) ŌĆó Amphetamine type : Amphetamine, Methamphetamine and Phenmetrazine. III. Drugs that cause only psychic dependence: ŌĆó Cocaine, LSD, Cannabis and Caffeine.
- 6. Drugs of abuse and their target receptors ŌĆóDrugs: ’āśOpiates ’āśCocaine ’āśNicotine ’āśEthanol ’āśAmphetamine ’āścannabinoids Receptor ŌĆóAgonists at mu, delta, and kappa receptors. ŌĆóIndirect agonist of dopamine by inhibiting its transporter ŌĆóNicotinic acetylcholine (Ach) receptors ŌĆóGABA agonist and NMDA receptor antagonist ŌĆóIndirect agonist of dopamine by stimulating its release ŌĆó CB1 and CB2 receptors
- 7. MESOLIMBIC PATHWAY ŌĆó Mesolimbic pathway ( reward pathway) is a dopaminergic pathway in the brain which connects ventral tegmental area located in the midbrain to the nucleus accumbens. ŌĆó The mesolimbic pathway releases dopamine into the nucleus accumbens and stimulates rewarding system. ŌĆó Abused drugs [alcohol, opiates, ╬ö9tetrahydrocannabinol (╬ö9- THC), and psychostimulants, including nicotine] interact with endogenous neural pathways in the brain. ŌĆó In particular, they share the common property of activating mesolimbic dopamine brain reward systems, and virtually all abused drugs elevate dopamine levels in the nucleus accumbens. ŌĆó In nucleus accumbens, ŌłåFosB functions as a master control protein in the development of drug addiction. ŌĆó Once it is overexpressed it triggers series of transcription events that ultimately produce an adaptive state.
- 10. CANNABIS (MARIJUANA) ŌĆó Cannabis is one of the oldest known psychoactive plant. ŌĆó It is obtained from the Hemp plants, Cannabis sativa Cannabis indica ŌĆó The active ingredients are present in the resinous exudate of the tops of the female plants. ŌĆó The psychoactive principle of cannabis is known as Ōłå-9- tetrahydrocannabinol (THC). ŌĆó Cannabinoids are less liable than opiates, nicotine and alcohol to cause dependence having long term psychological effects.
- 11. CANNABINOID RECEPTOR: ŌĆó ŌłåTHC acts on the CB1 (central) and CB2 (immune cells) cannabinoid receptors. ŌĆó Ligands for these receptors proteins include - Endocannabinoids (produced naturally in the body by animals) eg. Anandamide, 2- Arachidonoyl glycerol - Phytocannabinoids (found in the cannabis species) eg. Ōłå THC - Synthetic cannabinoids (manufactured artificially) eg. Naphthoylindole, Phenacetylindole. CB1 Receptor ŌĆó Location: Basal ganglia, limbic system, hippocampus, male and female reproductive systems, anterior eye and retina. ŌĆó Involved in dependence mechanism CB2 Receptor ŌĆó Location: Immune-derived cells, spleen, peripheral nervous system. ŌĆó Not involved in dependence mechanism
- 12. MECHANISM OF ACTION OF CANNABINOIDS ŌĆó CB1R is a G protein-coupled receptor located in the central and peripheral nervous system. ŌĆó Activated by the endocannabinoid neurotransmitters Anandamide and 2- Arachidonoyl glycerol or by THC. ŌĆó CB1R is linked via Gi protein it inhibits adenylate cyclase and voltage operated calcium channels and activates G-protein-sensitive inward-rectifying potassium channels(GIRK) causing hyperpolarization and inhibits neurotransmitter release. ŌĆó CB1R also influences gene expression both directly by activating mitogen-activated protein kinase and indirectly by reducing the activity of protein kinase A as a result of reduced adenylate cyclase activity.
- 14. MOLECULAR MECHANISM OF CANNABINOID DEPENDENCE: prolong exposure of cannabinoids on several components of the brain neuronal circuits lead to cause dependence via 1)Synaptic plasticity: ŌĆó Neuronal circuits and their elements undergo important adaptation due to addictive drugs by - Modulating the number and strength of neuron-neuron connections - Synaptic plasticity (the dynamic adjustment of synaptic efficacy occurring in response to environmental or internal stimuli) ŌĆó Endocannabinoids supresses presynaptic glutamate release leading to a depolarization-induced suppression of excitation(DSE) and inhibit presynaptic GABA release leading to depolarization suppression of inhibition (DSI), both effects lasts for 1 minute. ŌĆó THC acts via presynaptic CB1 receptor to inhibit release of glutamate and GABA in the striatum and cause long term form of synaptic plasticity like long term potentiation (LTP) and long term depression(LTD). This effect can last for hours or weeks.
- 15. 2) Changes in CB1R density and function: ŌĆó CB1R is coupled to G-proteins of the Gi class, which implies its activation and inhibits adenylate cyclase and voltage gated Ca++ channels and activate K+ channel and hinders synaptic transmission. ŌĆó Uncoupling and downregulation of brain CB1R after prolonged THC exposure plays key role in development of cannabinoid addiction and tolerance. ŌĆó Repeated THC exposure reduces coupling efficacy of CB1R to Gi transduction proteins, the receptors gets desensitized.
- 16. 3) Signalling cascades: ŌĆó The MAPK/ERK pathway is a chain of proteins in the cell that communicates a signal from a receptor on the surface of the cell to the DNA in the nucleus of the cell. ŌĆó The signal starts when a signalling molecule binds to the receptor on the cell surface and ends when the DNA in the nucleus expresses a protein and produces some change in the cell, such as cell division ŌĆó The members of the mitogen-activated protein kinase(MAPK) signalling system, such as MEK1/2, JNK(c-Jun N-terminal kinase)and ERK (extracellular signal regulated kinases) are major modulators of cell functions, including proliferation, differentiation and survival. ŌĆó Cannabinoids increase concentration of MAPK due to which this MAPK/ERK1/2 cascade pathway gets activated which alters gene expression.
- 17. signs of abuse/dependence ŌĆó Anger or Aggression ŌĆó Decreased Appetite / Weight Loss ŌĆó Irritability ŌĆó Nervousness / Anxiety ŌĆó Restlessness ŌĆó Sleep Difficulties / Strange Dreams
- 18. DRUGS USED FOR TREATMENT: ŌĆó Dronabinol (Acts as an agonist & It reduces symptoms of withdrawal syndrome and reduces use of cannabis) ŌĆó Encaptone (It is used to decrease cannabis cravings) ŌĆó Divalproex ŌĆó Buspirone ŌĆó Recent pre-clinical studies suggest the potential of FAAH inhibitors such as URB597, endocannabinoid metabolising enzymes