
































More Related Content
What's hot (20)
Similar to Dying with Dignity PP for reals.pptx (15)













Dying with Dignity PP for reals.pptx
- 1. Dying with Dignity Caroline L. Eckard DrOID COM225
- 2. Definitions • Death with dignity: “(1) an end-of-life option that allows certain eligible individuals to legally request and obtain medications from their physician to end their life in a peaceful, humane, and dignified manner; (2) state legislation codifying such an end-of-life option; (3) a family of organizations promoting the end-of-life option around the United States” (FAQs…). • Physician Assisted Death: a term often used interchangeably with physician-assisted suicide (PAS), which involves a doctor "knowingly and intentionally providing a person with the knowledge or means or both required to commit suicide, including counseling about lethal doses of drugs, prescribing such lethal doses or supplying the drugs” (CMA Policy…). • Euthanasia: “ knowingly and intentionally performing an act that is explicitly intended to end another person's life and that includes the following elements: the subject has an incurable illness; the agent knows about the person's condition; commits the act with the primary intention of ending the life of that person; and the act is undertaken with empathy and compassion and without personal gain” (CMA Policy…). • Three types of Euthanasia are identified; the divisions are premised on whether the subject has and expresses a desire to end their life: • Voluntary euthanasia is limited to situations where the subject is a competent, informed person who has voluntarily asked for his or her life to be ended. • Non-voluntary euthanasia means the person has not developed or expressed his or her preference regarding aid in dying or is incapacitated and is unable to make or exercise an informed choice. • In-voluntary euthanasia means the person made an informed choice and expressed his or her refusal for aid in dying.
- 3. PAS/PAD vs Euthanasia • involve the use of lethal medications to deliberately end a patient's life •the patient must self- administer the medications; the "aid-in- dying" refers to a physician providing the medications, but the patient decides whether and when to ingest the lethal medication •when a third party administers medication or acts directly to end the patient’s life Physician Aid in Dying/ Physician Assisted Suicide Euthanasia (Braddock III & Tonelli
- 4. Other Practices that are not PAS or PAD • Some other practices that should be distinguished from physician aid-in-dying include: ▪ Withholding/withdrawing life-sustaining treatments: When a competent adult patient makes an informed decision to refuse life-sustaining treatment, their wishes are generally respected. The right of a competent adult patient to refuse life-sustaining treatments is supported by law. ▪ Pain medication that may hasten death: Often a terminally ill, suffering patient may require dosages of pain medication that have side effects that may hasten death, such as impairing respiration. Using the ethical principle of double effect as the foundational argument, it is generally held by most professional societies, and supported in court decisions, that this action is justifiable. Since the primary goal and intention of administering these medications is to relieve suffering, the secondary outcome of potentially hastening death is recognized as an expected and acceptable side-effect in a terminally ill patient. ▪ Palliative sedation: This term refers to the practice of sedating a terminally ill patient to the point of unconsciousness, due to intractable pain and suffering that has been refractory to traditional medical management. Such patients are imminently dying, usually hours or days from death. Often other life-sustaining interventions continue to be withheld (CPR, respirator, antibiotics, artificial nutrition and hydration, etc.) while the patient is sedated. Palliative sedation may occur for a short period (respite from intractable pain) or the patient may be sedated until s/he dies. In the rare instances when pain and suffering is refractory to treatment even with expert clinical management by pain and palliative care professionals, palliative sedation may legally be employed.
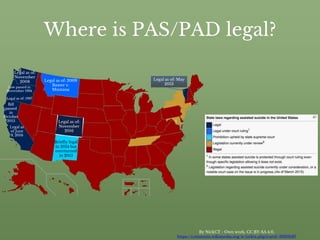
- 5. Where is PAS/PAD legal? By NickCT - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=39316187 Briefly legal in 2014 but overturned in 2015 Legal as of: 1997 Legal as of: November 2016 Legal as of: May 2013 Legal as of: November 2008 Legal as of: 2009 Baxter v. Montana Legal as of June 9, 2016 (As of March 2015) Bill passed in October 2015 Law passed in November 1994
- 6. States where there is no specific statute making assisted suicide illegal • Washington D.C. • Nevada (The act may or may not be covered by common law.) • North Carolina (The act may or may not be covered by common law.) • Utah (Utah does not recognize common law and has no specific statute for assisted suicide.) • West Virginia • Wyoming (Wyoming does not recognize common law and has no specific statute for assisted suicide.) (ProCon.org 2015)
- 7. Who Qualifies for PAS/PAD? •Must be a resident within one of the six states •Must be 18 years or older •Must have six months or less till expected death due to a terminal illness •Must have two oral (or least 15 days apart) and one written request to a physician •Must be capable of making and communicating health care decisions for him/herself and has made the request voluntarily (ProCon.org 2015)
- 8. Most Common Arguments Against Physician Aid-in- Dying: 1.Sanctity of life 2.Passive vs. Active distinction 3.Potential for abuse 4.Professional integrity 5.Fallibility of the profession
- 9. Argument #1: Sanctity of Human Life •Religious and secular traditions upholding the sanctity of human life have historically prohibited suicide or assistance in dying. PAD is morally wrong because it is viewed as diminishing the sanctity of life. (Braddock III & Tonelli 2013) • We are made in God’s image (Genesis 1:26–27) and therefore human life has an inherently sacred attribute that should be protected and respected at all times. While God gave humanity the authority to kill and eat other forms of life (Genesis 9:3), the murdering of other human beings is expressly forbidden, with the penalty being death (Genesis 9:6). (Old Testament vs New Testament)
- 10. Counter Argument to the “Sanctity of Human Life” • Not everyone has the same God or even believes in God(s), it is unfair to take away a choice because some people disagree • If the penalty for bloodshed is death - isn’t that just more bloodshed? • With the definition of “bloodshed” meaning: “(1) destruction of life, as in war or murder; slaughter; or (2) the shedding of blood by injury, wound, etc” (“bloodshed”). • If you take the second definition: There is no blood involved in PAD, the patient merely takes a few pills and falls asleep to die. • If you take the first definition: According to the United States Law, murder is “the killing of another human being under conditions specifically covered in law. In the U.S., special statutory definitions include: murder committed with malice aforethought, characterized by deliberation or premeditation or occurring during the commission of another serious crime, as robbery or arson (first-degree murder) and murder by intent but without deliberation or premeditation (second-degree murder)” (“murder”). Due to the fact that PAD is done without malicious intent and is done not by the physician but at the will of the patient to end their life merely with the aid of a physician, it should not be attributed to murder. • Furthermore, some physicians aid their patients in dying without even knowing it, usually prescriptions are given in monthly increments meaning you most likely will have 30 pills in one fill of the medication, if one were to take all 30 pills, they would most likely die or become extremely ill.
- 11. Argument #2: Passive vs. Active Distinction “There is an important difference between passively "letting die" and actively "killing." Treatment refusal or withholding treatment equates to letting die (passive) and is justifiable, whereas PAD equates to killing (active) and is not justifiable” (Braddock III & Tonelli 2013).
- 12. Counter Argument #2: Passive vs. Active Distinction • Both killing (active) and withholding treatment (passive) have the same result: the patient dies, the difference being that the person either dies quickly or slowly. • Furthermore, since the physician only supplies the patient with the script to ascertain the drugs, and does not administer them directly or lay a hand on the patient, it could be considered passive (accepting or allowing what happens or what others do, without active response or resistance). • Usually when one has a terminal illness, they are in extreme pain, sometimes the drugs do not work any more or they’re incapacitated or otherwise “not all there.” • In the event of being in extreme pain and knowing you won’t recover, would you rather have a quick and painless death or prolong your suffering to get to the same end result?
- 13. Argument #3: Potential for Abuse “Vulnerable populations, lacking access to quality care and support, may be pushed into assisted death. Furthermore, assisted death may become a cost-containment strategy. Burdened family members and health care providers may encourage loved ones to opt for assisted death and the protections in legislation can never catch all instances of such coercion or exploitation. To protect against these abuses, PAD should remain illegal.” (Braddock III & Tonelli 2013)
- 14. Counter Argument #3: Potential for Abuse • With all the restrictions in place for being allowed to participate in PAD, it is unlikely that one would be able to go through all avenues and requirements without arousing suspicion, and since the patient must communicate to the physician that he/she wishes to end their life, the only way one could possibly use this as a means to rid themselves of debt would be to either blackmail the patient into giving their consent or use a psychological tactic to convince the patient to give their consent (i.e. hypnotherapy, conditioning, door-in-face tactic, foot-in-door tactic, etc.).
- 15. Argument #4: Professional Integrity “Historical ethical traditions in medicine are strongly opposed to taking life. For instance, the Hippocratic oath states, "I will not administer poison to anyone where asked," and I will "be of benefit, or at least do no harm." Furthermore, some major professional groups such as the American Medical Association and the American Geriatrics Society oppose assisted death. The overall concern is that linking PAD to the practice of medicine could harm both the integrity and the public's image of the profession.” (Braddock III & Tonelli 2013)
- 16. Counter Argument #4: Professional Integrity • In the hippocratic oath one of the things physicians promise is to “remember that there is art to medicine as well as science, and that warmth, sympathy, and understanding may outweigh the surgeon's knife or the chemist's drug” (“Definition of Hippocratic Oath” 2016); if someone is in so much pain with no hope of survival or if they are aware they are going to die soon, don’t we owe it to them to give them their dying wish? Don’t we owe them sympathy and warmth, as physicians have promised? • “I will remember that I remain a member of society, with special obligations to all my fellow human beings, those sound of mind and body as well as the infirm” (“Definition of Hippocratic Oath” 2016); we owe it to the people we treat to remember that we are there to help them and whether helping is preventing someone from dying or helping them move on from this life so they can die with dignity surrounded by those who love them and on their own terms.
- 17. Counter Argument #4: Professional Integrity (continued) • “I will respect the privacy of my patients, for their problems are not disclosed to me that the world may know. Most especially must I tread with care in matters of life and death. If it is given me to save a life, all thanks. But it may also be within my power to take a life; this awesome responsibility must be faced with great humbleness and awareness of my own frailty. Above all, I must not play at God” (“Definition of Hippocratic Oath” 2016). Obviously this statement in itself is hypocritical, but it draws on the fact that physicians have the power to take a life as well as save it, or saving someone’s life by taking it; saving them from months of extreme agony, or not being able to move, eat, or breathe by themselves, being left in a vegetative state for the last few months of their so-called “life,” making their family watch them go through this pain and watch them slowly deteriorate with no hope of a comeback, it’s almost sick. • Furthermore, physicians are not required to take the hippocratic oath, it is optional and even if they do indeed decide to take the oath - they are in NO way bound by it.
- 18. Argument #5: Fallibility of the Profession “The concern here is that physicians will make mistakes. For instance there may be uncertainty in diagnosis and prognosis. There may be errors in diagnosis and treatment of depression, or inadequate treatment of pain. Thus the State has an obligation to protect lives from these inevitable mistakes and to improve the quality of pain and symptom management at the end of life.” (Braddock III & Tonelli 2013)
- 19. Counter Argument #5: Fallibility of the Profession • Mistakes are inevitable, however it is not the physician’s fault if someone wishes to end their life, people will do what they want to do, having PAD be legal benefits the patient, the physician and the family. It gives physicians more time to work on patients who still have the possibility of getting better; it allows the patient to die with dignity on their own terms and without being in excruciating pain; and it allows the family to grieve and remember their loved one as they were before instead as they are in that moment of agony. • I am uncertain as to why depression is mentioned since it is not a terminal illness, therefore it would not be allowed for the patient to participate in PAD
- 20. Brittany Maynard Born in Anaheim, California, on November 19, 1984. Graduated from the University of California, Berkeley with a bachelor's degree in psychology in 2006 from the College of Letters and Science and the University of California, Irvine School of Education in 2010 with a master's degree in education. Interested in international travel since high school (Maynard taught at orphanages in Kathmandu, Nepal and traveled also to Vietnam, Cambodia, and other Southeast Asian countries.) Married Daniel Esteban "Dan" Diaz in September 2012 and they were trying for a family. (Girap 2015)
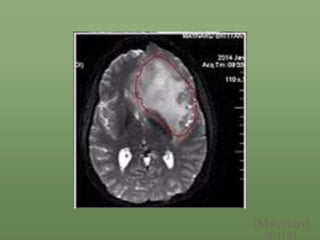
- 21. Brittany Maynard’s Debilitating Diagnosis & Death • On January 1, 2014, she was diagnosed with stage 2 astrocytoma and had a partial craniotomy and a partial resection of her temporal lobe. • The cancer returned in April 2014, and her diagnosis was then elevated to stage 4 astrocytoma with a prognosis of six months to live. • Moved from California to Oregon to take advantage of Oregon's Death with Dignity Law, saying she had decided that "death with dignity was the best option for me and my family." • Partnered with Compassion & Choices to create the Brittany Maynard Fund, which seeks to legalize aid in dying in states where it is now illegal. She also wrote an opinion piece for CNN titled "My Right to Death with Dignity at 29”. • On October 29, 2014, she stated that "it doesn't seem like the right time right now" but that she would still end her own life at some future point. • Planned to end her life on November 1, 2014, with drugs prescribed by her doctor. Maynard wrote in her final Facebook post: "Goodbye to all my dear friends and family that I love. Today is the day I have chosen to pass away with dignity in the face of my terminal illness, this terrible brain cancer that has taken so much from me ... but would have taken so much more."
- 22. (Maynard
- 23. My Mother’s Side of the Family (Most of us)
- 24. Maureen(20) & Frank(23) Muller’s Wedding November 22, 1952
- 25. Frank and Maureen Muller, 2009
- 26. References bloodshed. (n.d.). Dictionary.com Unabridged. Retrieved November 20, 2016 from Dictionary.com website http://www.dictionary.com/browse/bloodshed Braddock III, C. H., MD, MA, & Tonelli, M. R., MD, MA. (2013). Physician Aid-in-Dying: Ethical Topic in Medicine (H. Starks PhD, MPH, D. Dudzinski PhD, MTS, & N. White MD, MA, Eds.). Retrieved November 19, 2016, from http://depts.washington.edu/bioethx/topics/pad.html CMA POLICY: EUTHANASIA AND ASSISTED SUICIDE (UPDATE 2007). (2007). Canadian Medical Association Publications, Ottawa, Ontario, Canada. Definition of Hippocratic Oath - MedicineNet. (2016, May 13). Retrieved October 23, 2016, from http://www.medicinenet.com/script/main/art.asp?articlekey=20909 FAQs - Death With Dignity. (n.d.). Retrieved November 19, 2016, from https://www.deathwithdignity.org/faqs/ Johnson, K. (2009, August 31). Montana Court to Rule on Assisted Suicide Case. Retrieved November 19, 2016, from http://www.nytimes.com/2009/09/01/us/01montana.html Girap, S. (Ed.). (2015). Brittany Maynard. Retrieved November 20, 2016, from http://alchetron.com/Brittany-Maynard-993059-W Old Testament vs New Testament: Same God? (n.d.). Retrieved November 20, 2016, from http://www.bibleinfo.com/en/questions/god-old-testament-same- god-new-testament-0 Maynard, B. (2014, November 2). Brittany Maynard: My right to death with dignity at 29. Retrieved October 19, 2016, from http://www.cnn.com/2014/10/07/opinion/maynard-assisted-suicide-cancer-dignity/index.html murder. (n.d.). Dictionary.com Unabridged. Retrieved November 20, 2016 from Dictionary.com website http://www.dictionary.com/browse/murder ProCon.org. (2015, October 5). State-by-State Guide to Physician-Assisted Suicide. Retrieved from http://euthanasia.procon.org/view.resource.php?resourceID=000132