

































More Related Content
Similar to Endomyocardial biopsy - indications and techniques (20)
Recently uploaded (20)


















Endomyocardial biopsy - indications and techniques
- 1. z ENDOMYOCARDIAL BIOPSY UNDER GUIDANCE OF DR S S KOTHARI SIR DR POOJA VYAS MAAM DR SHARAD JAIN SIR DR KEWAL KANABAR SIR
- 2. z INTRODUCTION ’é¦ It is an established invasive procedure in most frequently used for the monitoring of heart transplant rejection. ’é¦ EMB also has a complimentary role to the clincal assessment in establishing the diagnosis of myocarditis, infiltrative disorders like storage disorders, amyloidosis, drug induced toxicities. ’é¦ Improvements in EMB technique, equipment and analysis method of sample have led to improvement in diagnostic precision.
- 3. z HISTORICAL ASPECTS ’é¦ Konno and Sakakibara first reported percutaneous EMB procedure using as bioptome with sharpened cusps by pinching since 1950. ’é¦ Caves and Schultz modified the Konno-sakakibara forceps to allow percutaneous biopsy through right IJV under local anesthesia. ’é¦ The long sheath technique developed in 1974 improved feasibility and safety, a flexible KingŌĆÖs college bioptome introduced by Richardson can be introduced through long sheath.
- 4. z
- 6. z INDICATIONS ’é¦ Heart transplant rejection surveillance ’é¦ Clinically suspected Myocarditis ’é¦ Cardiotoxicity of cancer therapy ’é¦ Unexplained ventricular arrhythmias, conduction disorder. ’é¦ Autoimmune disorders ’é¦ Tumours of the heart ’é¦ Restrictive cardiomyopathy
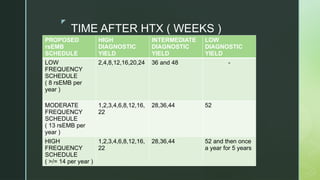
- 7. z TIME AFTER HTX ( WEEKS ) PROPOSED rsEMB SCHEDULE HIGH DIAGNOSTIC YIELD INTERMEDIATE DIAGNOSTIC YIELD LOW DIAGNOSTIC YIELD LOW FREQUENCY SCHEDULE ( 8 rsEMB per year ) 2,4,8,12,16,20,24 36 and 48 - MODERATE FREQUENCY SCHEDULE ( 13 rsEMB per year ) 1,2,3,4,6,8,12,16, 22 28,36,44 52 HIGH FREQUENCY SCHEDULE ( >/= 14 per year ) 1,2,3,4,6,8,12,16, 22 28,36,44 52 and then once a year for 5 years
- 8. z
- 9. z ACCESS SITE FOR PROCEDURE ’é¦ Right internal jugular vein is most common access site for right ventricular biopsy in heart transplant patients. ’é¦ Right femoral vein access is mostly used in non heart transplant patients. ’é¦ Right femoral artery and radial artery for LV EMB.
- 10. z SELECTION OF EMB SITE ’é¦ Most common site ŌĆō RV ’é¦ In suspected myocarditis and non ischemic cardiomyopathy including storage and infiltrative disorders biventricular EMB can increase diagnostic accuracy. ’é¦ It is suggested to take atleast 5 samples from different sites in RV and LV to reduce risk of sampling error. ’é¦ In patients of amyloidosis, abdominal fat pad biopsies have a sensitivity of 75% in AL amyloidosis, whereas sensitivity is lower in hereditary and ATTR type, thus a negative fat pad biopsy does not rule out cardiac involvement.
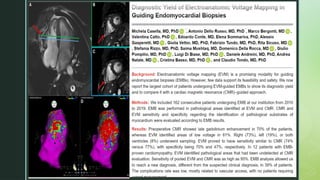
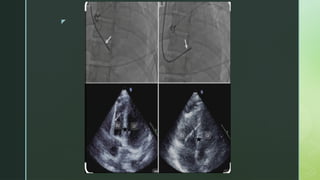
- 11. z IMAGING GUIDANCE ’é¦ EMB is mostly performed under fluoroscopic guidance. ’é¦ Pre procedural imaging like echo, cardiac MRI, PET can be used to direct site specific EMB ’é¦ Procedural imaging like echocardiography can be performed simultaneously with fluoroscopy to improve the accuracy of the EMB procedure. ’é¦ Intracardiac echo has also been successfully used to guide EMB of cardiac tumours. ’é¦ Electroanatomic voltage mapping is being used in diseases with focal pattern associated with VT ( sarcoidosis ), it is further facilitated with 3 D mapping.
- 12. z
- 13. z
- 14. z
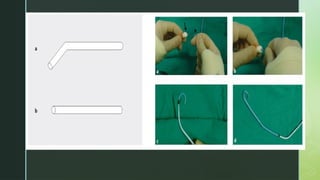
- 15. z BIOPSY TECHNIQUE RV BIOPSY ’é¦ VIA FEMORAL VEIN ’é¦ A short 5 Fr sheath is inserted in the femoral vein before the long preformed sheath is placed ’é¦ All preformed sheaths for RV EMB present an angulated distal end with an angle of curvature varying from 135-180 degree, whereas sheath for biopsy from LV apex is straight.
- 16. z
- 17. z ’é¦ Short sheath is replaced by a 5 F Ansel Cook 75 cm guiding sheath into the femoral vein and it is inserted into the right ventricular cavity with the assistance of an internal diameter and guidewire. ’é¦ With the insertion of bioptome in the preshaped long sheath, it may straighten the long preformed sheath, hence the distal portion of the unformed 104 cm bioptome can be manually preshaped. ’é¦ Preformed sheath with the pigtail is then introduced into the long cook sheath. ’é¦ Preformed sheath is guided into the RV by the use of guide wire, the guide wire is removed while sheath is remained in the position. ’é¦ After insertion of the preformed sheath it has to be continuously flushed to avoid clot formation, thromboembolic complication and air embolism.
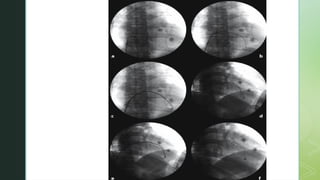
- 18. z ’é¦ The pigtail is removed after confirmation of tip of preformed sheath being directed towards the mid portion of the IVS. ’é¦ Performed sheath position can be confirmed by connecting pressure line to record RV pressure. ’é¦ On fluoroscopy, it should lie across the patients spine and is usually directed inferiorly. ’é¦ Further confirmation can be done in RAO 30 and LAO 60 whether catheter is on the ventricular side and facing towards the septum.
- 19. z
- 20. z ’é¦ Pigtail is then removed and 104 cm long bioptome is introduced in the preshaped sheath. ’é¦ Contact with the IVS is confirmed by PVC. ’é¦ Bioptome is withdrawn 1-2 cm, jaws are opened and advanced slowly to engage the septum. ’é¦ The biopsy head is slowly closed to encapsulate the endomyocardial specimen. ’é¦ Due to trabeculated nature of the surface, gentle forward pressure has to be maintained while jaws are closed.
- 21. z
- 22. z ’é¦ Patients with RCMP and post transplant often demonstrate pulsatile transmission of ventricular contractility through the bioptome, whereas those with DCMP are often soft and engagement is confirmed only by PVC. ’é¦ After the biopsy is taken, operator has to maintain pressure on forceps to make sure the jaws remain closed. ’é¦ There is light give away sensation as biopsy is taken and patient may infrequently may feel tugging sensation. ’é¦ Once removed, the specimen must be scooped using the small needle and saline and placed in the preservative.
- 23. z RIGHT IJV APPROACH ’é¦ After securing right IJV with a venous sheath,the preshaped 50 cm bioptome is introduced pointing towards the anterior wall of the right atrium. ’é¦ In the mid right atrium, the bioptome is advanced slowly with counterclockwise rotation. ’é¦ Continued rotation and slow advancement allow bioptome to enter into the right ventricle and orient towards the septum. ’é¦ If entry into the RV remains difficult , then a Swan Ganz catheter or other balloon floatation device may be used to define the pathway.
- 24. z
- 25. z LEFT IJV APPROACH ’é¦ Differenc from the right IJV is in the type of sheath used. ’é¦ 6F 10cm sheath is introduced in the left IJV, this sheath is exchanged over a 0.035 inch wire for a 6F 45 cm sheath. ’é¦ Under fluro guidance 45cm sheath is placed in RA. ’é¦ Bioptome is then introduced after removing a wire.
- 26. z LEFT VENTRICULAR BIOPSY ’é¦ Femoral artery approach requires insertion of a larger preformed sheath to maintain artery patency and allow biopsy sheath manipulation. ’é¦ The straight preformed sheath is inserted into the left ventricular cavity using a guide wire and a pig tail catheter. ’é¦ The wire, pig tail and sheath gently manipulated to cross the aortic valve and enter the LV ’é¦ The inferior posterior portion and areas of previous MI should be avoided to reduce the risk of perforation.
- 27. z ’é¦ The jaws are closed firmly with extraction of sample. ’é¦ Due to increased contraction of the Lv, less forward pressure is to be applied while performing the biopsy. ’é¦ The position of the sheath is maintained in the LV and its position is adjusted to ensure sampling from different sites.
- 28. z
- 29. z LV biopsy- Guiding catheter approach ’é¦ LV biopsy can also be performed using a 7F JR4 guiding catheter. ’é¦ To reach inferior, posterior, lateral and apical regions, JR4 is the best option. ’é¦ For anterior segment, AL1 catheter is better option. ’é¦ For left ventricular septum, JL4 is the best option ’é¦ The 105 cm bioptome is advanced through the guiding catheter.
- 30. z LV BIOPSY-RADIAL ARTERY SHEATHLESS APPROACH ’é¦ Availibity of low profile biptomes have made radial approach feasible. ’é¦ After heparinization and NTG pretreatment, 6F terrumo sheath is exchanged over a wire with 7.5 F sheathless multi purpose guiding catheter. ’é¦ Biopsy forceps is then inserted via a Y connector.
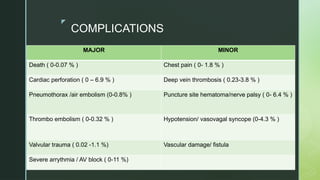
- 31. z COMPLICATIONS MAJOR MINOR Death ( 0-0.07 % ) Chest pain ( 0- 1.8 % ) Cardiac perforation ( 0 ŌĆō 6.9 % ) Deep vein thrombosis ( 0.23-3.8 % ) Pneumothorax /air embolism (0-0.8% ) Puncture site hematoma/nerve palsy ( 0- 6.4 % ) Thrombo embolism ( 0-0.32 % ) Hypotension/ vasovagal syncope (0-4.3 % ) Valvular trauma ( 0.02 -1.1 %) Vascular damage/ fistula Severe arrythmia / AV block ( 0-11 %)
- 32. z CARDIAC PERFORATION ’é¦ RV perforation common than LV ’é¦ Risk factors ’āś Patients with INR > 1.5 and has received heparin 2 hours prior to biopsy ’āś Pulmonary hypertension ’āś Bleeding diathesis ’āś RV enlargement.