





























Endoscopic Retrograde Cholangiopancreatography .pptx
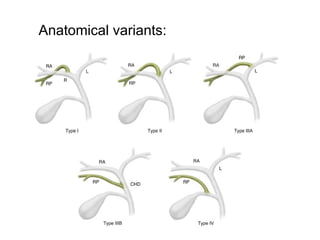
- 2. Anatomy of hepatobiliary system:
- 3. • Biliary anatomy parallels the portal venous supply of the liver. • The right hepatic duct drains the entire right lobe of the liver. It is formed by the union of the anterior right hepatic duct, which drains the anterior segments V and VIII, and the posterior right hepatic duct, which drains the posterior segments VI and VII. • The anterior right hepatic duct lies vertically, whereas the posterior hepatic duct is more horizontal . • The left hepatic duct is formed by the union of ducts draining segments II and III and one or more ducts from segment IV . • Segment I normally drains to both the left and the right hepatic ducts. • The bile ducts, together with branches of the hepatic artery and portal vein, form the portal triad.
- 5. • Endoscopic retrograde cholangiopancreatography (ERCP) is a diagnostic and interventional procedure technique using both endoscopy and fluoroscopy for examination and intervention of biliary tree and pancreatic ducts . • The standard technique for selective biliary cannulation, which is the first part of performing an ERCP, involves using a endoscope/duodenoscope and advancing this to the second part of the duodenum in a very similar manner to a conventional gastroscopy procedure.
- 6. Patient preparation: • Control film (AP/LAO of upper abdomen) • Report of USG/CT/MRI/Cholangiogram if available :To check opaque gall stones ,pancreatic calcifications/calculi. • May need antibiotics prior to ERCP. • A local anesthetic sprayed onto tongue /throat just before intubation. • May require sedation.
- 7. • Known allergic to iodine contrast:Pretreated with prednisone 40 mg for 3 days before exam. • Smooth muscle relaxant :Buscopan/atropine/glucagon given to reduce esophageal spasm and relax the sphincter of oddi for passage of endoscope and insertion of cannula .
- 8. Contrast media : • Non ionic tri-iodinated contrast agent : • Iapamidol,iohexol,iopramide,ioversol • Pancreatic duct :Low osmolar (1.5 mg /ml) • Bile duct :Low osmolar (2.8 mg/ml)
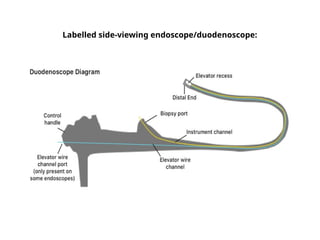
- 9. Equipment : • A side viewing fibre-optic endoscope • Polythene catheters. • Over couch/under couch X-ray tubes with tilting tables. • Fluoroscopic unit with spot film devices and image intensifier television system.
- 11. • Patient lies on left lateral /LAO position on the fluoroscopic table. • The initial process of ERCP involves esophageal intubation, navigation through the esophagus and stomach and entering the duodenum via the pylorus. • In the second part of the duodenum, the next step involves identifying the major papilla in the duodenum in order to perform biliary cannulation. • The first step involves positioning the duodenoscope so that the lens and working channel are located below the major papilla. • Once properly positioned, a sphincterotome or an alternative cannulation catheter is engaged into the orifice of the major duodenal papilla, aiming usually towards the 11 o’clock position in order to achieve common bile duct (CBD) cannulation. • Once suitably advanced, contrast injections can be given and this allows x- ray images to be obtained which can serve as a diagnostic test to look for pancreatobiliary pathology and also enable planning for any therapeutic interventions.
- 13. • Once the ampulla of vater is identified ,patient is turned prone to assist in selective cannulation of biliary duct . • It is easy to cannulate the pancreatic duct as it is straight in the papilla and the CBD is slightly angulated to the side.
- 14. • A polythene catheter prefilled with contrast media without any air bubble is introduced via the endoscope through the ampulla into distal end of CBD. • If failed try to introduce a guide wire into the papillary opening .Catheter is directed up the duct right over the guide wire. • Test injection of contrast under fluoroscopic guidance is made to determine the position of cannula . • Contrast is then injected to fill the biliary ducts and gall stones.
- 16. Film sequences : • Early bile duct filling films to show any calculi :Prone straight & prone oblique ,supine straight ,both obliques • Intrahepatic ducts:Trendelenberg position . • Lower end of CBD and gallbladder :Semi erect .
- 17. • Endoscope is removed to prevent obscuring the duct visualization and further radiographs are taken. • Delayed films of CBD and gallbladder are taken to evaluate emptying rate. • Usually four types of spot films are taken : • A)Initial scout • B)Initial cholangiogram. • C)Post procedure cholangiogram • D)Drainage film.
- 18. • For therapeutic ERCP ,special instruments are passed through the working channel of the endoscope that are used for cutting and opening into the bile duct ,stone removal ,dilatation of stricture and stent/drain placement .
- 19. Indications: • Biliary drainage. • Bile duct stones removal(choledocholithiasis). • Biliary stenting for strictures and leakage. • Biliary or pancreatic ductal system tissue sampling • Manometry for sphincter of oddi. • Balloon dilation of the duodenal papilla or ductal strictures. • Sphincterotomy ( sphincter of oddi dysfunction or stenosis). • Pre- or postoperative assessment of the biliary tree in patients undergoing laparoscopic cholecystectomy .
- 20. Contraindications Relative: • Altered anatomy in post-surgical states. • Structural abnormalities of esophagus, stomach or duodenum. • Unstable patient (severe cardiac/respiratory diseases). • Coagulopathy
- 27. Pancreatic Duct-Normal ERCP appearance.
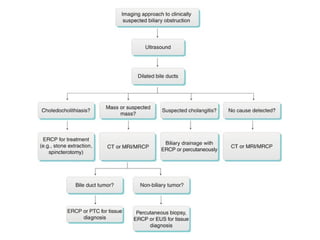
- 28. Causes of biliary dilatation
- 33. Biliary tract strictures from pancreatic carcinoma.
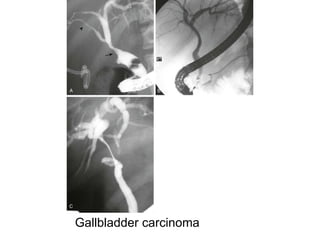
- 34. Cholangiocarcinoma appearances at ERCP.
- 36. Complications: • Pancreatitis (~5%) • Hemorrhage (2%) • Perforation leading to pneumoperitoneum and/or pneumoretroperitoneum(<1%) • Infection (cholangitis) • Migration of a biliary or pancreatic duct stent • complications secondary to endoscopy e.g. esophageal and gastric injury
- 37. Post-ERCP pancreatitis in a 50-year-old man.
- 38. Hemorrhage and perforation after ERCP in a 67- year-old woman.
- 39. Stent misplacement or migration
- 40. Thank you