epiaortic echocardiography in cardiac surgery
0 likes26 views

epiaortic echocardiography katz grading














































































More Related Content
Similar to epiaortic echocardiography in cardiac surgery (20)
More from Rajesh Munigial (18)
















Recently uploaded (20)




















epiaortic echocardiography in cardiac surgery
- 1. EPIAORTIC ECHOCARDIOGRAPHY Presenter : Dr Rajesh Munigial DM First Year Trainee Dept Of Cardiac Anaesthesiology JNMC , Belgaum
- 2. Topics Of Discussion ŌĆó Introduction ŌĆó Indications ŌĆó stroke ŌĆó Probes and technique ŌĆó Imaging planes ŌĆó Atherosclerotic plaque grading
- 3. INTRODUCTION ŌĆó Epiaortic ultrasound (EAU) is an imaging modality whereby a handheld transducer is placed directly upon a surgically exposed aorta ŌĆó EAU provides high-quality sonographic data depicting aortic anatomy and pathology ŌĆó Epicardial ultrasound was used in the 1980s at The Mount Sinai Medical Center and at Columbia University College of Physicians and Surgeons
- 4. Epiaortic ultrasound is a useful tool to assess diseased aorta, especially during its manipulation or instrumentation like ’üČaortic clamp placement and removal, ’üČ insertion of the aortic cannula, ’üČthe antegrade cardioplegia vent, ’üČthe proximal anastomosis of coronary grafts, ’üČaortotomy ŌĆó It can identify diseased aortic segments containing atherosclerotic plaque, calcification, or thrombus that are at high risk for distal embolization ŌĆó It also helps in risk stratification for patients at risk of complications from distal embolization
- 5. ŌĆó Perioperative stroke is a major cause of morbidity and mortality in the cardiac surgery population Incidence : Off-pump CABG: 1.9% On pump CABG:3.8% Aortic valve surgery: 4.8% Mitral valve surgery: 8.8% Combined CABG and valve surgery:7.4%
- 6. Risk Factors For stroke in cardiac surgery Include : ŌĆó Advanced age ŌĆó Female gender ŌĆó Proximal aortic atherosclerosis ŌĆó Calcified aorta ŌĆó History of cerebrovascular disease ŌĆó Peripheral vascular disease ŌĆó Diabetes ŌĆó Hypertension ŌĆó Prior cardiac surgery ŌĆó Preoperative infection (including endocarditis), ŌĆó Urgent surgery ŌĆó Greater than 2-hour cardiopulmonary bypass (CPB) time, ŌĆó Intraoperative hemofiltration, and transfusion The presence of aortic plaque correlates well with postoperative stroke incidence. The more extensive and complex the plaque burden, the higher the risk of postoperative stroke
- 7. POSSIBLE MECHANISM OF STROKE : ’āśArterial to arterial embolization of plaque or thrombus ’āśEmbolization from intracardiac sources ’āśParadoxical embolization from venous to arterial (through intra or extra-cardiac shunts ) ’āśIschemic injury due to arterial thrombosis ’āśAir entrainment ’āśCerebral hemorrhage ’āśDecreased cerebral venous drainage ’āśProlonged seizure activity
- 8. Manipulation Of Aorta SANDBLASTING EFFECT
- 9. Intraoperative-3 methods of detection of plaque and calcificataion Surgical palpation of aorta ŌĆōLEAST SENSITIVE Transesophageal echocardiography EPIAORTIC ultrasound-MOST SENSITIVE
- 10. INDICATIONS OF EAU ŌĆó Increased risk of embolic stroke ŌĆó History of cerebrovascular disease ŌĆó Peripheral vascular disease ŌĆó Other imaging modalities demonstrating atherosclerosis It is recommende d to use in patients with
- 11. WHY EPIAORTIC ULTRASOUND ?? Easy to use Minimal time to perform Negligible complication rate High accuracy Provides direct and dynamic visualisation during surgery Surgical palpation is subjective
- 12. EAU SUPERIOR TO TEE ŌĆó Most surgical manipulation: in the region of ascending aorta (BLIND SPOT FOR TEE) (where the trachea and left mainstem bronchus interpose between the esophagus and aorta, causing disruption of ultrasound transmission) ŌĆó TEE unable to image the greatest area of interest of ascending aorta ŌĆó EAU is closer to the area of interest ŌĆó Enabling high transducer frequencies ŌĆ”high quality images with fewer artifacts
- 13. How EAU alters surgical management Off pump CABG (as opposed to on pump ) No touch techniques Alteration in site of aortic instrumentation/manipulation Aortic endarterectomy/ aortic arch replacement
- 14. DISADVANTAGES Of EAU ŌĆó Need for sterility---potential for surgical field contamination ŌĆó Potential to cause arrythmias
- 16. PROBES AND TECHNIQUE ŌĆó Handheld transducer , sheathed in sterile covering , placed directly on ascending aorta with or without standoff ŌĆó Standoff refers to the distance between the probe and the object of interest Because of the wedge shape of the image, if the transducer is placed directly on the aorta, the anterior aortic wall (near field) will not be completely imaged; only a small section will be displayed while the rest will be outside the sector. To capture the near field in its entirety, the transducer is held at some distance away from the aorta (the standoff) This requires addition of a medium that conducts ultrasound waves-gel
- 17. Three types of probes available for imaging Linear probe ŌĆō rectangular image Phased array ŌĆōwedge shaped image Matrix array ŌĆōwedge shaped image
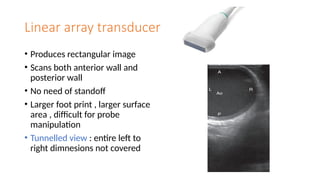
- 18. Linear array transducer ŌĆó Produces rectangular image ŌĆó Scans both anterior wall and posterior wall ŌĆó No need of standoff ŌĆó Larger foot print , larger surface area , difficult for probe manipulation ŌĆó Tunnelled view : entire left to right dimnesions not covered
- 19. Phased array transducer ŌĆó Ideally >7MHZ ŌĆó Small footprint ŌĆó Simultaneous left and right walls imaging ŌĆó Kept at a distance of 1cm away from aorta ŌĆó Need for standoff
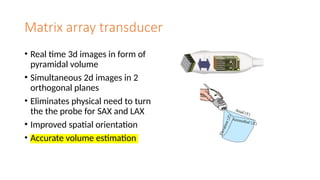
- 20. Matrix array transducer ŌĆó Real time 3d images in form of pyramidal volume ŌĆó Simultaneous 2d images in 2 orthogonal planes ŌĆó Eliminates physical need to turn the the probe for SAX and LAX ŌĆó Improved spatial orientation ŌĆó Accurate volume estimation
- 21. IMAGING PLANES ŌĆó Most recent guidelines recommend 5 standard views to complete a comprehensive EAU examination from the sinotubular junction to the innominate artery and aortic arch. ŌĆó The ascending aorta is divided into proximal, mid-, and distal segments. ŌĆó Each segment of the ascending aorta can be described as having four walls: anterior (near field), posterior (far field), right, and left ŌĆó This leaves 12 total wall segments of the ascending aorta to characterize.
- 22. Proximal ascending aorta: beginning of STJ , where it is common to see aortic valve and right pulmonary artery Mid ascending aorta: Defined by the part of the aorta that is juxtaposed with the right pulmonary artery Distal ascending aorta: from the distal right pulmonary artery to the innominate artery. More distally : proximal aortic arch
- 23. Short Axis Examination ŌĆó The ultrasound probe is positioned on the ascending aorta as proximally as possible, with the orientation marker directed toward the patientŌĆÖs left shoulder. ŌĆó A significant difference between the antero-posterior and medial-lateral dimensions is an indicator of an orthogonal view. ŌĆó Measurements made in such a plane will be inaccurate. ŌĆó After identifying the proximal ascending aorta, where it is frequently possible to image the aortic valve, slowly advancing the probe distally in a cephalad direction along the aorta permits visualization of the mid ascending aorta, and finally the distal ascending aorta toward the aortic arch at the origin of the innominate artery. ŌĆó During the transit toward the innominate artery, it is necessary to rotate the probe in a clockwise fashion to maintain the SAX orientation. Advancing the probe slightly further permits examination of the proximal aortic arch
- 26. Epiaortic ultrasonographic image of the normal ascending (Asc) aorta in short-axis view obtained with phased-array transducer. Aortic wall areas that can be imaged in short axis include anterior (A), posterior (P), right lateral (RL), and left lateral (LL) walls. PA, Pulmonary artery; SVC, superior vena cava
- 27. LONG AXIS EXAMINATION ŌĆó The LAX orientation is achieved by rotating the probe 90 degrees from the SAX orientation . ŌĆó Proximally, the sinus of Valsalva, sinotubular junction, and aortic valve can be visualized ŌĆó The probe is then advanced in cephalad direction ŌĆó The aortic arch, with origins of the left common carotid and left subclavian artery, should be located as a final part of the examination
- 28. ŌĆó Epiaortic ultrasonographic image and accompanying diagram of normal ascending (Asc) aorta in long-axis view obtained with phased-array transducer. Aortic wall areas that can be imaged include anterior (A) and posterior (P) walls in each of proximal, mid, and distal segments. RPA, Right pulmonary artery
- 32. Doppler interrogation of ascending aorta and aortic valve ŌĆó Use of EAU for Doppler interrogation of the aortic valve is limited. ŌĆó In some cases, color Doppler may be useful to diagnose the presence or absence of dissections and hematomas. ŌĆó EAU has been used to guide aortic cannulation of patients with type A aortic dissections. ŌĆó In these cases, use of 2D EAU and color Doppler EAU helped identify true and false channels for successful arterial cannulation of the true lumen
- 33. ŌĆó It is difficult to obtain Doppler beam orientation parallel to aortic flow in many parts of the ascending aorta because more frequently than not, the orientation of the ultrasound probe to flow in the aorta will be perpendicular ŌĆó One must be careful to recognize that there is an element of error when the Doppler beam is not parallel to the direction of flow. ŌĆó The angle between the Doppler beam and the direction of flow within the aorta is called the insonation angle. ŌĆó It should be less than 30 degrees to maintain an error of less than 15%.
- 35. SUMMARY OF RECOMMENDATIONS ŌĆó 5 views for evaluation : 3 SAX(proximal,mid and doistal ascending aorta) , 1 LAX of ascending aorta and 1 LAX of proximal aortic arch ŌĆó 3 measurements to be recorded for each of 3 ascending aorta sax view and aortic arch 1. Maximal plaque height/thickness 2. location of the maximal plaque within the ascending aorta; and 3. presence of mobile components The maximal aortic diameter in SAX may also be recorded
- 36. ŌĆó Verbal report to be provided to surgical team before aortic manipulation ŌĆó written report documenting examination findings should be available in the patientŌĆÖs chart within 24 hours of completion of the examination ŌĆó Trainees in perioperative echocardiography should participate in the evaluation of 25 EAU examinations, at least 5 of which must be personally directed by the individual under the direct supervision of an echocardiographer with advanced level training
- 44. REFERENCES 1. Glas KE, Swaminathan M, Reeves ST, Shanewise JS, Rubenson D, Smith PK, Mathew JP, Shernan SK; Council for Intraoperative Echocardiography of the American Society of Echocardiography; Society of Cardiovascular Anesthesiologists. Guidelines for the performance of a comprehensive intraoperative epiaortic ultrasonographic examination: recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists; endorsed by the Society of Thoracic Surgeons. J Am Soc Echocardiogr. 2007 Nov;20(11):1227-35. doi: 10.1016/j.echo.2007.09.001. PMID: 17983940. 2. KaplanŌĆÖs cardiac anaesthesia perioperative and critical care
- 50. Thank you !!!