ER Management of Acute Asthma Attack
•Download as PPTX, PDF•
7 likes•2,039 views

This document discusses the management of acute asthma attacks. It begins by describing the symptoms of mild to moderate versus severe asthma exacerbations. It then discusses principles and goals of care, which include relieving airflow limitation, treating inflammation and hypoxemia/hypercapnia. Early treatment at home with a written asthma action plan and recognition of worsening symptoms is emphasized. The document also discusses pre-hospital, emergency department and inpatient management, as well as adjunctive therapies such as heliox, magnesium sulfate and bronchial thermoplasty.














ER Management of Acute Asthma Attack
- 1. ER Management of Acute Asthma Attack Ahmed Al Gahtani, BSRC, RRT Associate Director, Clinical Education Respiratory Therapy Program Inaya Medical College
- 2. Asthma exacerbations consist of acute or sub-acute episodes of: Coughing Wheezing Progressively worsening SOB Chest Tightness Combination
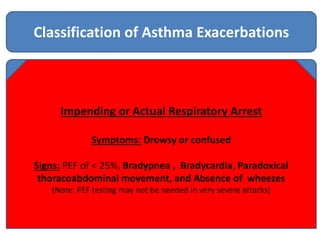
- 3. Impending or Actual Respiratory Arrest Classification of Asthma Exacerbations SevereMild to Moderate Mild to Moderate Exacerbation Symptoms: SOB while at rest, prefers sitting, talk in phrases, and/or usually agitated. Signs: PEF of ≥ 40%, Increased RR, HR 100 to 120 , use of accessory muscles, loud wheezes throughout exhalation, PaO2 ≥ 60 mm Hg and/or PaCO2 < 42 mm Hg, SpO2 90 to 95 % Severe Exacerbation Symptoms: SOB while at rest, Sits upright, talk in wards, and usually agitated. Signs: PEF of < 40%, Increased RR often > 30, HR > 120 , usually uses accessory muscles, loud wheezes throughout inhalation & exhalation, PaO2 < 60 mm Hg and/or PaCO2 ≥ 42 mm Hg, SpO2 < 90 % Impending or Actual Respiratory Arrest Symptoms: Drowsy or confused Signs: PEF of < 25%, Bradypnea , Bradycardia, Paradoxical thoracoabdominal movement, and Absence of wheezes (Note: PEF testing may not be needed in very severe attacks)
- 4. Early treatment of asthma exacerbations is the best strategy for management. Important elements of early treatment at the patient’s home include a written asthma action plan; recognition of early signs and symptoms of worsening The NAEPP Expert Panel recommends that all clinicians treating asthmatic patients should be prepared to treat an asthma exacerbation, recognize the signs and symptoms of severe and life- threatening exacerbations, and be familiar with the risk factors for asthma- related death. Because infants are at greater risk for respiratory failure, clinicians should also be familiar with special considerations in the assessment and treatment of infants experiencing asthma exacerbations.
- 5. Principles and Primary Goals of Care • Relieve airflow limitation • Treat airway inflammation • Treat hypoxemia or hypercapnia if present. • Non-invasive ventilation / mechanical ventilation in severe cases (clinical judgment). • Selected therapies: magnesium sulphate and heliox. • Limited or no role for antibiotics and methylxanthines (aminophylline/theophylline).
- 6. Management Pre-Hospital Management EMSAt Home All EMS personnel should receive training in how to respond to the signs and symptoms of severe airway obstruction and impending respiratory failure
- 10. Expert Panel Report 3: National Heart Lung and Blood Institute 2007 https://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf
- 17. • Heliox • Antibiotics • Systemic Aminophylline • Magnesium Sulfate • Bronchial Thermoplasty Adjunct Therapies Am J Respir Crit Care Med. 2012 Apr 1;185(7):709-14
- 19. References • PROCEEDINGS OF THE AMERICAN THORACIC SOCIETY VOL 6 2009Thank You