Factsheet 1
âĒ
0 likesâĒ192 views

This document provides instructions for setting up and using a Graseby MS26 syringe driver for palliative care. It describes how to draw up medication, set the rate, label and secure the syringe, insert the cannula, and monitor the syringe driver. Regular checks of the syringe driver are important to ensure correct operation and identify any issues like blockages or leaks. Seeking specialist advice is recommended if any problems arise.




Factsheet 1
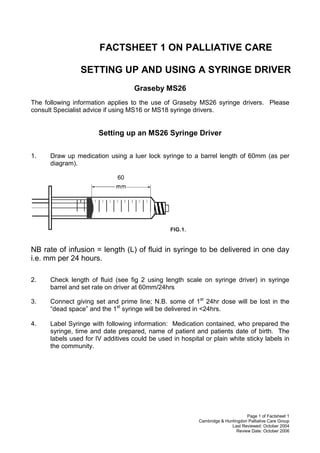
- 1. Page 1 of Factsheet 1 Cambridge & Huntingdon Palliative Care Group Last Reviewed: October 2004 Review Date: October 2006 FACTSHEET 1 ON PALLIATIVE CARE SETTING UP AND USING A SYRINGE DRIVER Graseby MS26 The following information applies to the use of Graseby MS26 syringe drivers. Please consult Specialist advice if using MS16 or MS18 syringe drivers. Setting up an MS26 Syringe Driver 1. Draw up medication using a luer lock syringe to a barrel length of 60mm (as per diagram). FIG.1. NB rate of infusion = length (L) of fluid in syringe to be delivered in one day i.e. mm per 24 hours. 2. Check length of fluid (see fig 2 using length scale on syringe driver) in syringe barrel and set rate on driver at 60mm/24hrs 3. Connect giving set and prime line; N.B. some of 1st 24hr dose will be lost in the âdead spaceâ and the 1st syringe will be delivered in <24hrs. 4. Label Syringe with following information: Medication contained, who prepared the syringe, time and date prepared, name of patient and patients date of birth. The labels used for IV additives could be used in hospital or plain white sticky labels in the community. 60
- 2. Page 2 of Factsheet 1 Cambridge & Huntingdon Palliative Care Group Last Reviewed: October 2004 Review Date: October 2006 FIG. 2. 5. Insert battery into the driver. The battery compartment is in the back of the driver and has a sliding cover. An alarm sounds for a few seconds when the battery is inserted correctly. Press and hold down the start/boost button. The motor will run for about 8 seconds at the end of which the alarm will sound until button released. (While the motor is running you can feel the lead screw turning) Release start button. The driver is now running. The indicator light should now be flashing (one flash in 25 secs), if it is not flashing change the battery. Each battery will last for about 50 deliveries. There is no stop button on the driver, remove battery to stop. 6. šÝšÝßĢ actuator back as far as it will go. Position the syringe in the driver. The flange of the syringe fits into a slot on the top of the driver - see FIG.2. The syringe plunger needs to be fitted into the driver actuator by pressing the white button and sliding the actuator along until it rests securely against the end of the plunger - see FIG.3. FIG.3. Flange and Slot Plunger Actuator
- 3. Page 3 of Factsheet 1 Cambridge & Huntingdon Palliative Care Group Last Reviewed: October 2004 Review Date: October 2006 7. Secure the syringe in position with the rubber securing strap (Fig. 2). 8. šÝšÝßĢ the plastic cover over the driver (the plastic cover must be placed so that the hole is aligned with boost button). 9. Insert cannula subcutaneously (wherever possible use Teflon avoiding metal). DO NOT SITE IN OEDEMATOUS AREAS. Upper chest or upper arms are best site (avoid upper arm if adjacent to breast surgery). 10. Connect giving set to cannula, (if not already attached). 11. Cover site with semi permeable film dressing and secure tubing with non-allergenic tape. 12. Check site and rate of infusion regularly. If there are signs of inflammation re-site, and change the giving set. 13. When the drug infusion has completed, or the prescribed drug dosage is altered, draw up drugs in a new syringe and insert as before, then label: there is no need to change the line. As long as the battery has not been removed there is no need to press the start/boost button. The alarm will sound: âĒ Immediately after battery insertion âĒ On holding the boost button down for >9 seconds âĒ When syringe has discharged âĒ If cannula blocked or line kinked âĒ If malfunction Remember:- âĒ Always use a luer lock syringe. âĒ Always set the Rate of Administration at 60mm/24hrs. âĒ Some of the first 24hr dose will be lost in the âdead spaceâ resulting in the contents of the first syringe being delivered in <24 hours. âĒ Always check drug compatibility (refer to Factsheet No. 3). Never mix more than 3 drugs in a syringe, with the exception of antisecretory agents (refer to factsheet No. 3). ANY PROBLEMS SEEK SPECIALIST ADVICE. The Attending Doctor Must Prescribe:- 1. Each drug to be used in the syringe and its 24 hour dose. 2. Driver setting of 60mm/24hrs. 3. The diluent (WATER OR SODIUM CHLORIDE 0.9% FOR INJECTION) volume.
- 4. Page 4 of Factsheet 1 Cambridge & Huntingdon Palliative Care Group Last Reviewed: October 2004 Review Date: October 2006 4. Where symptoms are uncontrolled a bolus stat dose of medication should be prescribed to be administered at the time of commencement of the syringe driver. 5. Appropriate âprnâ subcutaneous doses of each drug contained within the syringe also to be prescribed. The Administration Record The nursing staff have responsibility for the administration record. The date and start time for each syringe as well as the dose of each drug must be documented. The site viability should be assessed prior to starting a new syringe. Syringe driver check is to be carried out regularly and documented. Avoid subcutaneous pump in patients with bleeding tendency (seek advice). Monitoring Syringe Drivers in Use Regular checks on syringe driver operation must be built into the daily nursing routine. They should include checks for:- âĒ Signs of precipitation in the syringe âĒ Correct rate of administration âĒ Volume of drugs left in the syringe Integrity of the administration line, cannula and syringe driver Why NOT to use the âBoostâ Facility: The Graseby MS26 syringe driver incorporates a âBoost Buttonâ. If pressed a small bolus dose of the drugs in the syringe to be administered. 1 press of the boost button = 0.25mm travel (1 /240 th total daily dose) THE USE OF THE BOOST BUTTON IS NOT RECOMMENDED AS THE DOSE DELIVERED IS NOT A THERAPEUTIC DOSE. If the Boost Button is used - Remember:- âĒ Extra doses of all drugs in the syringe will be given. âĒ The non-therapeutic dose administered will be insufficient to control symptoms and should be used as a sign that the prescription may need to be amended. âĒ Repeated use of the boost button will result in the syringe lasting <24hrs. âĒ For appropriate additional dose see Factsheet 2.
- 5. Page 5 of Factsheet 1 Cambridge & Huntingdon Palliative Care Group Last Reviewed: October 2004 Review Date: October 2006 Syringe driver trouble shooting 1. Driver not functioning: Flat battery Battery in wrong way round Blocked cannula Start/Boost button not pressed 2. Driver functioning but light not flashing: Battery low 3. Alarm sounding: Syringe empty Kinked tubing/cannula blocked Driver malfunction 4. Infusion too slow: ?Site inflamed/cannula blocked ?Tubing kinked ?Syringe and tubing still connected ?Syringe plunger accurately in place 5. Infusion too fast: Check rate setting and calculation 6. Inflammation at cannula site: Infection/inflammation. Re-site cannula and change giving set 7. Recurrent site inflammation: Review drugs; ?reduce concentration of irritant drug ?change to alternative drug Seek Specialist Advice N.B. Patient and/or carers should be instructed how to replace battery. A spare battery should be left at the house. IF IN DOUBT SEEK SPECIALIST ADVICE