First Part.MA.Oct202010
âĒDownload as PPT, PDFâĒ
1 likeâĒ235 views

First part of meta-analysis lecture, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Convert to study materialsBETA
Transform any presentation into ready-made study materialâselect from outputs like summaries, definitions, and practice questions.




![AVAILABILITY OF INFORMATION
Summary effects only (OR, RR, HR, mean [SD]). Most of
the cases â Limited analyses.
What to do? Contact authors, Patient level data
Meta-analysis l
October 10, 2012 l](https://image.slidesharecdn.com/firstpartmaoct202010-13498428040234-phpapp02-121009232241-phpapp02/85/First-Part-MA-Oct202010-21-320.jpg)

First Part.MA.Oct202010
- 1. Meta-analysis Adrian V. Hernandez, M.D., Ph.D. Assistant Professor of Medicine Quantitative Health Sciences October 21, 2010
- 2. OUTLINE FIRST PART (40 minutes) Introduction, objectives, types of meta-analysis, definition of research question, getting information, inclusion/exclusion criteria Break 10 minutes Meta-analysis l October 10, 2012 l
- 3. OUTLINE (2) SECOND PART: 50 MINUTES âĒ Analysis (models, methods, heterogeneity, publication bias, quality, subgroup analysis) âĒ Reporting of meta-analysis (PRISMA, MOOSE guidelines) Meta-analysis l October 10, 2012 l
- 4. META-ANALYSIS: FACTS âĒ Too much information is available âĒ Many meta-analyses published lately: 1989-1993: 1301 1994-1998: 2532 1999-2003: 4917 2004-2008: 10567 âĒ Why meta-analyses? Saves money and effort Evaluates limitations of the evidence Designs future research Provides evidence for regulatory processes Meta-analysis l October 10, 2012 l
- 5. OBJECTIVES âĒ Summarize and integrate results of studies âĒ Analyze differences among studies âĒ Overcome small sample sizes âĒ Increase precision of effects âĒ Evaluate effects in subsets of patients âĒ Generate new hypotheses Meta-analysis l October 10, 2012 l
- 6. TYPES OF META-ANALYSES âĒ Randomized controlled trials (RCTs) âĒ Observational Studies âĒ Diagnostic studies Meta-analysis l October 10, 2012 l
- 7. CRITICAL ISSUES âĒ Identification and selection of studies âĒ Heterogeneity of results âĒ Analysis of data âĒ Reporting of results âĒ Interpretation of published results Meta-analysis l October 10, 2012 l
- 8. IDENTIFICATION AND SELECTION OF STUDIES âĒ The most critical step of a meta-analysis âĒ Clearly specified in protocol âĒ Phases: 1. Definition of research question 2. Literature search 3. Choice of relevant studies Meta-analysis l October 10, 2012 l
- 9. DEFINITION OF RESEARCH QUESTION âĒ Are the beneficial and harmful effects of glycoprotein IIb/IIIa receptor blockers similar between younger and older NSTE-ACS patients? âĒ What is the risk of HF with the use of rosiglitazone and pioglitazone in patients at high risk of DM and with type 2 DM? âĒ Which are the risk factors associated with hypercapnia in obese patients with OSA and without COPD? Meta-analysis l October 10, 2012 l
- 10. LITERATURE SEARCH âĒ Pubmed-Medline (www.pubmed.gov) âĒ Embase (www.embase.com) âĒ Ovid-Medline (www.ovid.com) âĒ The Web of Science (isiknowledge.com) âĒ Cochrane Library (www.cochrane.org) âĒ Scopus (www.scopus.com) âĒ Google Scholar (scholar.google.com) More on: Steinbrook R. NEJM 2006; 354:4-7. Meta-analysis l October 10, 2012 l
- 11. LITERATURE SEARCH - BIASES âĒ Publication bias âĒ Search bias âĒ Selection bias Meta-analysis l October 10, 2012 l
- 12. PUBLICATION BIAS Positive results are more likely to be published than negative results Meta-analysis l October 10, 2012 l
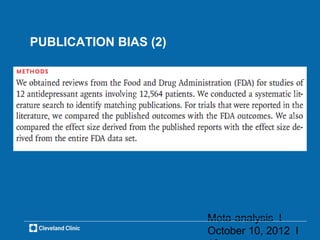
- 13. PUBLICATION BIAS (2) Meta-analysis l October 10, 2012 l
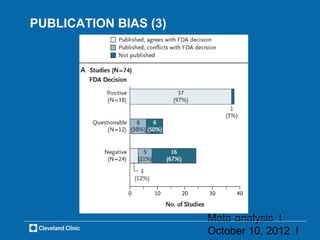
- 14. PUBLICATION BIAS (3) Meta-analysis l October 10, 2012 l
- 15. PUBLICATION BIAS (4) How to avoid/diminish? âĒ Identify unpublished studies (e.g. Nissen SE et al. NEJM 2007) âĒ Search registries (e.g. NIHâs http://clinicaltrials.gov) âĒ Do not discard studies in other languages (e.g. German, French, Spanish) Meta-analysis l October 10, 2012 l
- 16. SEARCH BIAS How happens? Limited number of search engines Inappropriate keywords How to avoid/diminish? âĒ At least 3 search engines âĒ Use relevant keywords and show them (e.g. for RCTs: see Dickersin K et al. BMJ 1994; 309: 1286-91) âĒ Two or more researchers Meta-analysis l October 10, 2012 l
- 17. SELECTION BIAS How happens? Long list of potential articles Selection necessary (similarity, -replication) How to avoid/diminish? âĒ Define clear list of inclusion and exclusion criteria âĒ Two or more researchers Meta-analysis l October 10, 2012 l
- 18. INCLUSION/EXCLUSION CRITERIA âĒ Objective âĒ Population studied âĒ Study design-Quality of data âĒ Sample size âĒ Treatment/Intervention âĒ Controls âĒ Duration of study âĒ Calendar time Meta-analysis l October 10, 2012 l
- 19. J Gastrointest Surg (2009) 13:649â656 DOI 10.1007/s11605-008-0756-8 Inclusion: phase III RCTs, Gum chewing vs. control (active/placebo) on time to flatus/LOS, elective colorectal surgery for localized disease (cancer or not), open or laparoscopic, >15 years, English, 1960-2008. Exclusion: Non-randomized studies, surgery beyond colorectal, prior colonic surgery, emergency surgery. Meta-analysis l October 10, 2012 l
- 20. COMBINATION OF STUDIES ALWAYS POSSIBLE? Enough info?, quality?, heterogeneity? Meta-analysis l October 10, 2012 l
- 21. AVAILABILITY OF INFORMATION Summary effects only (OR, RR, HR, mean [SD]). Most of the cases â Limited analyses. What to do? Contact authors, Patient level data Meta-analysis l October 10, 2012 l
- 22. ALL STUDIES CAN BE COMBINED? Only reasonably well conducted RCTs? Observational studies also? Similar results between RCTs and observational? Similar results overtime? Meta-analysis l October 10, 2012 l
- 23. MA OF RCTs vs. OBSERVATIONAL âĒ 3 RCTs, n=10731 diabetic/high risk of diabetes, >12 months f-up: OR 2.1 (95% CI: 1.1-4.1) âĒ 4 Retrospective cohorts, n=67382 diabetic patients: OR 1.6 (95% CI 1.3-1.8) Meta-analysis l October 10, 2012 l
- 24. MAs OVERTIME: OBSERVATIONAL (1) 17 studies (3C, 14CC) RR for ischemic stroke: 2.8 (95%CI 2.2-3.4) Cohorts: 3.2 (2.0-5.3) Case-control: 2.8 (2.2-3.5) Meta-analysis l October 10, 2012 l
- 25. MAs OVERTIME: OBSERVATIONAL (2) 20 studies (4C, 16CC) RR for all-stroke: 1.9 (95%CI 1.4-2.6) Cohorts: 1.0 (0.5-1.8) Case-control: 2.1 (1.6-2.9) RR for ischemic stroke: 2.7 (95%CI 2.2-3.4) Meta-analysis l October 10, 2012 l