Global Perspectives on Pharmaceutical Anti-Counterfeiting
•Download as PPTX, PDF•
1 like•828 views

A presentation given at a recent conference in the USA. It looks at the global issues involved in pharmaceutical anti-counterfeiting, pointing out the problems involved in scaling up what is proposed in USA and Europe into a global drug tracking system.





















Global Perspectives on Pharmaceutical Anti-Counterfeiting
- 1. Mark Davison © John Steven Hernandez
- 2. Agenda ď‚— What are the global issues? ď‚— What anti-counterfeiting technologies could work everywhere? ď‚— How do we best serve developing countries? ď‚— What do the patients want? mark.davison@bluespherehealth.com 2
- 3. No Man is an Island… mark.davison@bluespherehealth.com 3
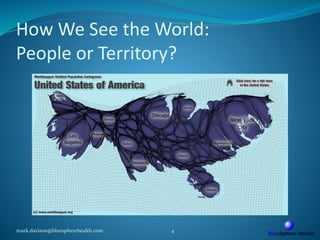
- 4. How We See the World: People or Territory? mark.davison@bluespherehealth.com 4
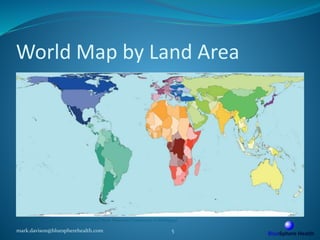
- 5. World Map by Land Area mark.davison@bluespherehealth.com 5 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 6. “Headline” Counterfeit Flows mark.davison@bluespherehealth.com 6 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 7. Response: Logistics-Based Security  Control the product flow, control the crime…  Serialization, pedigree, RFID etc.  Tech-centric approaches  Infrastructure requirements  Pay-offs in patient safety, logistics efficiency  Reduces opportunity for large-scale crime  Provides a modular, scalable, global framework mark.davison@bluespherehealth.com 7
- 8. Deadliest Counterfeit Flows mark.davison@bluespherehealth.com 8 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 9. “Internal”Counterfeits mark.davison@bluespherehealth.com 9 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 10. Logistics is Only One Aspect  Tech-centric approaches are difficult in developing countries  Doesn’t deal with locally-produced fakes  Wider approach is needed mark.davison@bluespherehealth.com 10
- 12. Global Share of Land… mark.davison@bluespherehealth.com 12 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 13. … Share of Population mark.davison@bluespherehealth.com 13 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 14. …and Share of Poverty mark.davison@bluespherehealth.com 14 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 15. Who Pays the Costs of Anti-Counterfeiting? “The costs associated with implementing E-pedigree will be too high for some California pharmacists to absorb. This means even more small business pharmacies will be put in jeopardy. This will harm patient access to prescription drugs and consultation care.” National Community Pharmacists Association, Dec 2007 http://www.pharmacy.ca.gov/meetings/minutes/2007/07_dec_enf1.pdf mark.davison@bluespherehealth.com 15
- 16. Who Pays the Costs of Anti-Counterfeiting? “The costs associated with implementing E-pedigree will be too high for some California pharmacists to absorb. This means even more small business pharmacies will be put in jeopardy. This will harm patient access to prescription drugs and consultation care.” National Community Pharmacists Association, Dec 2007 http://www.pharmacy.ca.gov/meetings/minutes/2007/07_dec_enf1.pdf mark.davison@bluespherehealth.com 16
- 17. Who Pays the Costs of Anti-Counterfeiting? “The costs associated with implementing E-pedigree will be too high for some California pharmacists to absorb. This means even more small business pharmacies will be put in jeopardy. This will harm patient access to prescription drugs and consultation care.” National Community Pharmacists Association, Dec 2007 http://www.pharmacy.ca.gov/meetings/minutes/2007/07_dec_enf1.pdf mark.davison@bluespherehealth.com 17 #8 GDP Worldwide. If California cant afford it, who can?
- 18. “Ubiquitous Anti-Counterfeiting Technology” Must Be:  Secure  Easy to use with minimal / no training  Physically robust  Low entry costs (or subsidized)  Flexible and scalable  Upgradable and Replaceable mark.davison@bluespherehealth.com 18
- 20. Role of the State ď‚— Centralized solutions may be the best option ď‚— Europe, USA, China, Brazil etc. ď‚— Not all states will cope with serialization ď‚— Heavy subsidy and technical help needed ď‚— Scalable approaches to aid phased uptake ď‚— Supportive, non-punitive environment mark.davison@bluespherehealth.com 20
- 21. But… Share of Public Health Spending mark.davison@bluespherehealth.com 21 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
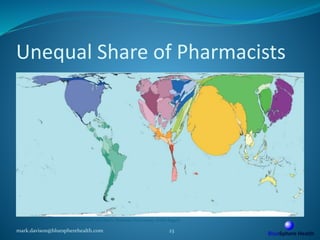
- 22. How About the Pharmacist? ď‚— The last professional to touch the pack ď‚— Trained and trainable (in anti-counterfeiting systems) ď‚— Ubiquitous in every community? mark.davison@bluespherehealth.com 22
- 23. Unequal Share of Pharmacists mark.davison@bluespherehealth.com 23 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 24. Publicly-funded Healthcare and Private Pharmacists mark.davison@bluespherehealth.com 24 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan) Mostly private-sector pharmacists Pharmacists Public funding
- 25. Pharmacy-Based Drug Security ď‚— Relatively simple, logical approach ď‚— May not work everywhere ď‚— Not all pharmacists are equivalent ď‚— Sometimes they are the problem not the solution mark.davison@bluespherehealth.com 25
- 26. How About the Consumer?  Ubiquitous  Least trained element of the supply chain  Most to lose if product security fails:  We invest, but they ingest  Very effective if given the right systems  Communication is vital:  Education, education, education  Should only be the “sentinel of last resort” against fake drugs mark.davison@bluespherehealth.com 26
- 27. How to get the message across to consumers?
- 28. Share of Literacy mark.davison@bluespherehealth.com 28 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
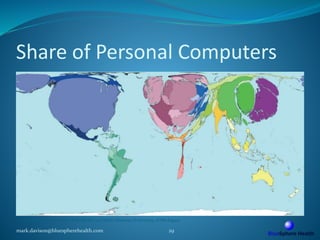
- 29. Share of Personal Computers mark.davison@bluespherehealth.com 29 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 30. Share of Languages mark.davison@bluespherehealth.com 30 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan)
- 31. Consequences  Low literacy levels and high language diversity need to be dealt with and planned for  Don’t assume that the message transmitted is the message received  Adapt materials and channels to local requirements  Culture, language, taboos etc  Use verbal communication when necessary:  Radio, local networks, village meetings  Reinforce the message repeatedly and frequently mark.davison@bluespherehealth.com 31
- 32. Clue: They don’t care about anti-counterfeiting technologies… mark.davison@bluespherehealth.com 32
- 33. Patients Want Safe Medicines ď‚— Supply chain security is vital ď‚— Customer is a useful last link for security ď‚— Many people are too poor to have choices ď‚— Choice of fake or real may actually be drug or no drug ď‚— Distinctions are often blurred ď‚— Traditional medicine versus western drugs ď‚— Expensive versus cheap ď‚— Genuine versus fake mark.davison@bluespherehealth.com 33
- 34. Why Don’t Drug Companies Just Concentrate on Keeping Developed Markets Safe?  Serialize (code) everything but only check a subset  Developed countries, Major urban centres  Protect (paying) patients’ health, share price, revenues  Eliminate the costs and complexity of a global system! mark.davison@bluespherehealth.com 34 “Devil’s Advocate” question!
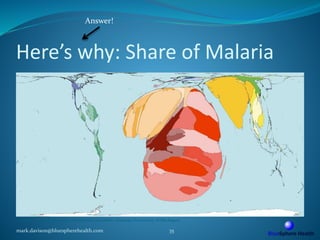
- 35. Here’s why: Share of Malaria mark.davison@bluespherehealth.com 35 © SASI Group (University of Sheffield) and Mark Newman (University of Michigan) Answer!
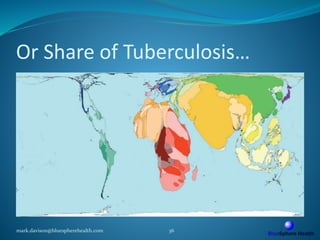
- 36. Or Share of Tuberculosis… mark.davison@bluespherehealth.com 36
- 37. “Fake tuberculosis and malaria drugs alone are estimated to kill 700,000 people a year. That’s equivalent to four fully laden jumbo jets crashing every day.” Julian Harris, International Policy Network, 2009 www.policynetwork.net/health/publication/keeping-it- real-protecting-worlds-poor-fake-drugs mark.davison@bluespherehealth.com 37
- 38. The World is Small, Disease Travels and Everyone is Connected mark.davison@bluespherehealth.com 38
- 39. Send me an email if you want to know more about global anti-counterfeiting issues. Photo on title slide by John Steven Fernandez www.flickr.com/photos/stevenfernandez/2069638117/ Maps are from Worldmapper.org and Buckminster Fuller Institute Any man's death diminishes me, For I am involved in mankind. And therefore never send to know For whom the bell tolls; It tolls for thee. (John Donne) mark.davison@bluespherehealth.com 39