Use of Glycated Hemoglobin (A1C) in the Diagnosis of Type 2 Diabetes Mellitus in Adults
ŌĆóDownload as PPTX, PDFŌĆó
1 likeŌĆó1,559 views

The Canadian Diabetes Association reviewed the use of glycated hemoglobin (A1C) for diagnosing diabetes and recommends adding it as a diagnostic criterion. An A1C level of 6.5% or higher confirms a diagnosis of diabetes. A1C testing has advantages over glucose tests as it can be done at any time and reflects average glucose levels over several months. However, A1C levels may be affected by certain medical conditions and ethnic groups. The document provides guidelines on using A1C for diagnosis and confirms the use of traditional glucose tests remain valid options.

Use of Glycated Hemoglobin (A1C) in the Diagnosis of Type 2 Diabetes Mellitus in Adults
- 1. Use of Glycated Hemoglobin (A1C) in the Diagnosis of Type 2 Diabetes Mellitus in Adults Shahid Nawaz Malik Researcher KSU
- 2. Ronald M. Goldenberg1 MD FRCPC FACE, Alice Y.Y. Cheng2 MD FRCPC, Zubin Punthakee3 MD FRCPC, Maureen Clement4 MD CCFP 1-North York General Hospital and LMC Endocrinology Centres, Toronto, Ontario 2-Division of Endocrinology & Metabolism, St. MichaelŌĆÖs Hospital and Credit Valley Hospital and Department of Medicine, University of Toronto, Toronto, Ontario 3-Department of Medicine and Department of Pediatrics, McMaster University, Hamilton, Ontario 4-University of British Columbia, Vancouver and Diabetes Education Centre, Vernon Jubilee Hospital, Vernon, British Columbia
- 3. The Canadian Diabetes Association (CDA) reviewed the use of glycated hemoglobin (A1C) in the diagnosis of diabetes mellitus. An International Expert Committee, the American Diabetes Association, a joint statement from the American Association of Clinical Endocrinologists/American College of Endocrinology, and a World Health Organization Consultation each recommend an A1C of 6.5% or higher as a criterion for the diagnosis of diabetes (1-4). The relationship between A1C and retinopathy is similar to that of fasting plasma glucose (FPG) or 2-hour plasma glucose (2hPG) with a threshold at around 6.5% (5-8). Although the diagnosis of diabetes is based on an A1C threshold for developing microvascular disease, A1C is also a continuous cardiovascular risk factor and a better predictor of macrovascular events than FPG or 2hPG (9,10).-
- 4. While many people identified as having diabetes using A1C ,will not be identified as having diabetes by traditional glucose criteria, and vice versa, there are several advantages to using A1C for diabetes diagnosis (4). - A1C can be measured at any time of day and is more convenient than FPG or 2-hour oral glucose tolerance test (OGTT). -A1C testing also avoids the problem of day- to-day variability of glucose values, as it reflects the average plasma glucose over the previous 2 to 3 months (2).
- 5. -In order to use this diagnostic criterion, A1C must be measured using a validated assay standardized to the National Glycohemoglobin Standardization ProgramŌĆöDiabetes Control and Complication Trials reference. It is important to note that A1C may be misleading in individuals with various hemoglobinopathies, iron deficiency, hemolytic anemias, and severe hepatic and renal disease (2,3,11) (Table 1).
- 6. In addition, studies of various ethnicities indicate that African Americans, American Indians, Hispanics and Asians have A1C values up to 0.4% higher than white patients at similar levels of glycemia (12,13). Further research is required to determine if specific ethnic-based A1C cut- points for diabetes diagnosis are warranted. A1C values are also affected by age, rising by up to 0.1% per decade (14-16). More studies may help determine if age-adjusted A1C thresholds are required for diabetes diagnosis in the elderly.
- 7. The CDA recommends the addition of A1C as a diagnostic criteria for type 2 diabetes in adults as follows: 1. A1C can be used as a diagnostic test for diabetes using a standardized, validated assay when there are no conditions that preclude its accurate measurement. 2. A1C Ōēź6.5% is one of the diagnostic criteria for diabetes that should be confirmed by repeat testing on a subsequent day. 3. A1C <6.5% does not exclude diabetes that may be diagnosed using standard glucose tests (Table 2). 4. Traditional diagnosis using FPG, random glucose with symptoms, or 2hPG during an OGTT are still recommended options for diagnosing diabetes (Table 2).
- 8. 5. A1C is not recommended for diagnostic purposes in children, adolescents, pregnant women or people with type 1 diabetes. 6. A1C may be misleading and therefore should not be used as a diagnostic tool in the setting of hemoglobinopathies, hemolytic anemia, thalassemias, iron deficiency, spherocytosis, and severe hepatic or renal failure. 7. A1C may be misleading in certain ethnicities and in the elderly, and therefore its utility as a diagnostic tool in these populations is unclear
- 9. The decision as to which test to use for diabetes diagnosis (Table 2) is left to clinical judgment. In the absence of unequivocal hyperglycemia accompanied by acute metabolic decompensation, a repeat confirmatory laboratory test (FPG, casual PG, 2hPG in a 75-g OGTT, A1C) must be done in all cases on another day. It is preferable that the same test be repeated for confirmation. If results of two different tests are available, and both are above the diagnostic cut-points, the diagnosis of diabetes is confirmed. When results of more than one test are available and are discordant, the test with a result above the diagnostic cut-point should be repeated and the diagnosis made on the basis of the repeat test
- 10. The CDA does not recommend specific A1C criteria for the diagnosis of prediabetes. While there is a continuum of risk for diabetes with A1C levels <6.5%, further research is required to determine whether A1C can be used to identify people at risk for diabetes (currently comprising people with impaired fasting glucose or impaired glucose tolerance).
- 11. 2hPG = 2-hour plasma glucose FPG = fasting plasma glucose OGTT = oral glucose tolerance test PG = plasma glucose
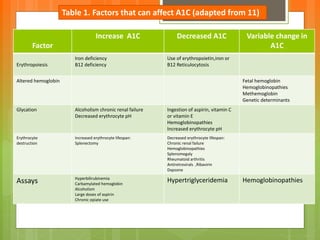
- 12. Factor Increase A1C Decreased A1C Variable change in A1C Erythropoiesis Iron deficiency B12 deficiency Use of erythropoietin,iron or B12 Reticulocytosis Altered hemoglobin Fetal hemoglobin Hemoglobinopathies Methemoglobin Genetic determinants Glycation Alcoholism chronic renal failure Decreased erythrocyte pH Ingestion of aspirin, vitamin C or vitamin E Hemoglobinopathies Increased erythrocyte pH Erythrocyte destruction Increased erythrocyte lifespan: Splenectomy Decreased erythrocyte lifespan: Chronic renal failure Hemoglobinopathies Splenomegaly Rheumatoid arthritis Antiretrovirals ,Ribavirin Dapsone Assays Hyperbilirubinemia Carbamylated hemoglobin Alcoholism Large doses of aspirin Chronic opiate use Hypertriglyceridemia Hemoglobinopathies Table 1. Factors that can affect A1C (adapted from 11)
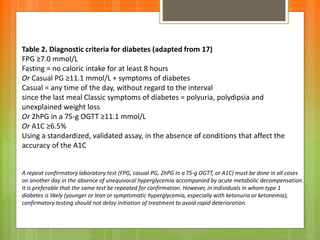
- 13. Table 2. Diagnostic criteria for diabetes (adapted from 17) FPG Ōēź7.0 mmol/L Fasting = no caloric intake for at least 8 hours Or Casual PG Ōēź11.1 mmol/L + symptoms of diabetes Casual = any time of the day, without regard to the interval since the last meal Classic symptoms of diabetes = polyuria, polydipsia and unexplained weight loss Or 2hPG in a 75-g OGTT Ōēź11.1 mmol/L Or A1C Ōēź6.5% Using a standardized, validated assay, in the absence of conditions that affect the accuracy of the A1C A repeat confirmatory laboratory test (FPG, casual PG, 2hPG in a 75-g OGTT, or A1C) must be done in all cases on another day in the absence of unequivocal hyperglycemia accompanied by acute metabolic decompensation. It is preferable that the same test be repeated for confirmation. However, in individuals in whom type 1 diabetes is likely (younger or lean or symptomatic hyperglycemia, especially with ketonuria or ketonemia), confirmatory testing should not delay initiation of treatment to avoid rapid deterioration.