Hearing Loss
âĒDownload as PPTX, PDFâĒ
1 likeâĒ475 views

Evaluation and Treatment






![Audiometry 101:
âĒ Interpret these results:
âĒ Mild-Moderate HL (cannot
hear <30 dB)
âĒ Bilateral HL = Normal
Weber
âĒ BC>AC = Conductive HL
âĒ Repeat test after treatment
[ ] = Bone Conduction
X O = Air Conduction](https://image.slidesharecdn.com/hearingloss-140718181558-phpapp01/85/Hearing-Loss-9-320.jpg)




![Audiometry 201:
âĒ Interpret these results:
âĒ Sloping high frequency HL
âĒ Bilateral HL = Normal
Weber
âĒ AC>BC = Positive Rene
âĒ Treatment options?
[ ] = Bone Conduction
X O = Air Conduction](https://image.slidesharecdn.com/hearingloss-140718181558-phpapp01/85/Hearing-Loss-16-320.jpg)




Hearing Loss
- 1. âCan You Hear Me Now?â Evaluation & Treatment of Hearing Loss Devon M. Fagel Ambulatory Clerkship January 14, 2010
- 2. Learning Objectives âĒ Understand epidemiology of hearing loss âĒ Review relevant anatomy and pathophysiology âĒ Describe the differential diagnosis for hearing loss âĒ Identify primary care patients at risk for hearing loss âĒ Evaluate hearing loss based on history and physical âĒ Interpret audiometry results and learn when to refer âĒ Select the most appropriate treatment for hearing loss
- 3. Epidemiology âĒ Third most prevalent chronic condition (28 million Americans). âĒ 40% of the population age 65 and older is hearing impaired. âĒ 65% of patients over 75 and 80% of those over 85 have HL. âĒ Prevalence of age-adjusted HL drastically risen since 1960s. âĒ Significant association between hearing loss and depression. âĒ 9% of internists offer hearing testing to patients over 65. âĒ 25% of patients with treatable HL receive hearing aids. Cruickshanks et al., Am J Epidemiol 148: 879-886, 1998 Wallhagen et al., Am J Public Health 87: 440-442, 1997 Yueh et al., JAMA 289: 1976-1985, 2003
- 4. Anatomy Yueh et al., JAMA 289: 1976-1985, 2003
- 5. Conductive vs. Sensorineural * Hearing defects affecting both ears will produce normal results. Conductive Hearing Loss Sensorineural Hearing Loss Anatomical Site Middle Ear Tympanic Membrane Inner Ear Inner Ear Cranial Nerve VIII Central Processing Center Weber Test* Sound localizes to affected ear Sound localizes to normal ear Rinne Test Negative = BC>AC (Bone/Air Gap) Positive = AC>BC Both decreased equally
- 6. Case #1 âĒ CC: âTrouble having a conversation, especially in noisy placesâ âĒ HPI: Patient reports difficulty understanding people in social situations. Having particular problems on the phone. Friends and family mention they often have to repeat themselves. Symptoms have become progressively worse over past few weeks. âĒ PE: Pt speaks very loudly. Negative Rinne (BC>AC), Weber normal. Unable to perform otoscopic exam (you forgot to charge the battery). âĒ What kind of hearing loss? Differential diagnosis?
- 7. Differential (Conductive Hearing Loss) âĒ Mechanical âĒ Cerumen: Most common cause of CHL (30% of elderly). âĒ Foreign body: Common objects include ear plugs, pencil tips. âĒ Infectious âĒ Otitis externa (swimmerâs ear): âĒ Common causes include cotton swabs, polluted water. âĒ Otitis media (glue ear): âĒ Common in children (shorter horizontal Eustacian tube). âĒ Destructive âĒ Cholesteatoma: Keratinizing squamous epithelium. âĒ Otosclerosis: Abnormal growth of bone near middle ear.
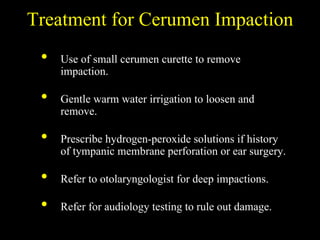
- 9. Audiometry 101: âĒ Interpret these results: âĒ Mild-Moderate HL (cannot hear <30 dB) âĒ Bilateral HL = Normal Weber âĒ BC>AC = Conductive HL âĒ Repeat test after treatment [ ] = Bone Conduction X O = Air Conduction
- 10. What is the primary diagnosis?
- 11. Treatment for Cerumen Impaction âĒ Use of small cerumen curette to remove impaction. âĒ Gentle warm water irrigation to loosen and remove. âĒ Prescribe hydrogen-peroxide solutions if history of tympanic membrane perforation or ear surgery. âĒ Refer to otolaryngologist for deep impactions. âĒ Refer for audiology testing to rule out damage.
- 12. Audiometry 101:
- 13. Case #2 âĒ CC: âDepressionâ âĒ HPI: 78 yo M reports feeling depressed and socially isolated after wife passed away last year. No longer talks to brother on the phone. Nearly arrested last week after getting into argument with Walmart cashier. Accused him of yelling and screaming at her. Spends most of the day watching TV (daughter complains too loud). âĒ PMH: CAD, CHF, CRI, HTN, DM, GERD, Low-back pain. âĒ SH: Retired airport mechanic, 50 pack-year smoker. âĒ Meds: Oxycodon, Lasix, Asparin. âĒ PE: BMI 35. Positive Rinne (AC>BC), Weber normal. Otoscopic exam unremarkable. âĒ Is there hearing loss? What evidence? Differential diagnosis?
- 14. Screening for Hearing Loss in Primary Care 0-8 = 13% probability 10-24 = 50% probability 26-40 = 84% probability
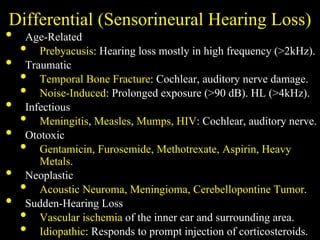
- 15. Differential (Sensorineural Hearing Loss) âĒ Age-Related âĒ Prebyacusis: Hearing loss mostly in high frequency (>2kHz). âĒ Traumatic âĒ Temporal Bone Fracture: Cochlear, auditory nerve damage. âĒ Noise-Induced: Prolonged exposure (>90 dB). HL (>4kHz). âĒ Infectious âĒ Meningitis, Measles, Mumps, HIV: Cochlear, auditory nerve. âĒ Ototoxic âĒ Gentamicin, Furosemide, Methotrexate, Aspirin, Heavy Metals. âĒ Neoplastic âĒ Acoustic Neuroma, Meningioma, Cerebellopontine Tumor. âĒ Sudden-Hearing Loss âĒ Vascular ischemia of the inner ear and surrounding area. âĒ Idiopathic: Responds to prompt injection of corticosteroids.
- 16. Audiometry 201: âĒ Interpret these results: âĒ Sloping high frequency HL âĒ Bilateral HL = Normal Weber âĒ AC>BC = Positive Rene âĒ Treatment options? [ ] = Bone Conduction X O = Air Conduction
- 18. Treatment for Presbyacusis Size Completely in Canal In Canal In Ear Behind Ear Cost Digital $1500-$4000 Analog Programable $1000-$2000 Analog Non- Programmabl e $700- $1500 Technolog y Remote Volume Control Directional Microphones Programmabilit y Analog vs DigitalBogardus et al., JAMA 289: 1986-1990, 2003
- 19. Case #3 âĒ CC: âFell on sidewalkâ âĒ HPI: 47 yo F presents to urgent care after falling and hitting her head on the pavement. She reports 1 week of nausea/vomiting. Husband states that she has been âstumblingâ lately. She also complains of HA which are getting progressively worse. Pt reports tinnitus in left ear and though left handed has been using rt hand to talk on the phone. âĒ PE: Positive Rinne (AC>BC), Weber lateralizes rt. Otoscopic exam unremarkable. âĒ What kind of hearing loss? Differential diagnosis?
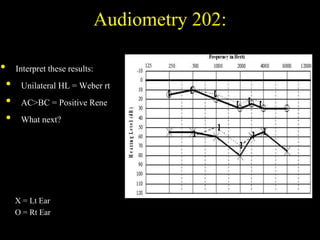
- 20. Audiometry 202: âĒ Interpret these results: âĒ Unilateral HL = Weber rt âĒ AC>BC = Positive Rene âĒ What next? X = Lt Ear O = Rt Ear
- 21. Unilateral Sensorineural Hearing Loss:
- 22. Recap: âĒ Covered epidemiology of hearing loss âĒ Covered anatomy and pathophysiology âĒ Covered differential diagnosis for hearing loss âĒ Covered primary care patients at risk for hearing loss âĒ Covered evaluation of hearing loss (history and physical) âĒ Covered interpretation of audiometry testing results âĒ Covered most appropriate treatment for hearing loss
Editor's Notes
- #4: - Third only to hypertension and arthritis (how many of you have treated HTN, arthritis, hearing loss?) - Almost half population of 65 (how many of you have treated those over 65?) - HL rising drastically (Why? iPods can deliver 115 dB) (Noise-induced hearing loss begins at 90 dB) - How many have asked about depression?
- #5: - Outer part of the ear (Pinna) collects sound. - Sound pressure is amplified through canal (middle ear) and transmitted to the cochlea via the tympanic membrane. - Air is contained in the outer and middle ear but not the inner, as TM moves, the Stapes transmits to the cochlea. - Inner ear is hollow, embedded in the temporal bone (densest bone of the body). - Chochlea contains sensory epithelium studded with hair cells (mechanoreceptors) which move with the fluid causing them to fire. - Sound is thus transformed into nerve impulses and delivered via CN 8 traveling through the brain stem to the temporal lobe.
- #7: What indicates hearing loss? Any clues as to what kind?
- #8: Cholesteatoma and Otosclerosis can eventually presents as mixed conductive/sensorineural
- #9: Normal hearing between 20 and -10 dB. Human speech occurs between 60 and 20 dB. Certain sounds have higher frequencies thus with certain types of HL may not be able to hear F, S, Th but no problem with M, N, O.
- #13: Normal hearing, common as we age that one ear is slightly better than other especially at higher frequencies. Here the lt ear is better than right. Possibly due to rt handed person and years of phone use.
- #14: Atherosclerosis may diminish vascularity of cochlea. What are indications of athlerosclerosis. High BMI Diabetes may causes vasculitis and endothelial proliferation in blood vessels of cochlea, reducing blood supply. Hypertension - vascular changes Ototxic drugs Smoking - accentuate atherosclerotic changes Noise trauma - airport mechanic Explain why Weber is normal?
- #16: Given pt info what is he at risk for - -Age-related, noise-induced, Ototoxic (Lasix, Asparin, Oxy) - Vascular ischemia
- #20: Did fall cause hearing loss or something else cause the fall? Explain Webere lateralizing rt (towards unaffected ear)