
![HIGH ALTITUDE SICKNESS 3[1].ppt](https://image.slidesharecdn.com/highaltitudesickness31-230905155430-23668e28/85/HIGH-ALTITUDE-SICKNESS-3-1-ppt-2-320.jpg)

![HIGH ALTITUDE SICKNESS 3[1].ppt](https://image.slidesharecdn.com/highaltitudesickness31-230905155430-23668e28/85/HIGH-ALTITUDE-SICKNESS-3-1-ppt-11-320.jpg)
![HIGH ALTITUDE SICKNESS 3[1].ppt](https://image.slidesharecdn.com/highaltitudesickness31-230905155430-23668e28/85/HIGH-ALTITUDE-SICKNESS-3-1-ppt-12-320.jpg)

![HIGH ALTITUDE SICKNESS 3[1].ppt](https://image.slidesharecdn.com/highaltitudesickness31-230905155430-23668e28/85/HIGH-ALTITUDE-SICKNESS-3-1-ppt-18-320.jpg)
![HIGH ALTITUDE SICKNESS 3[1].ppt](https://image.slidesharecdn.com/highaltitudesickness31-230905155430-23668e28/85/HIGH-ALTITUDE-SICKNESS-3-1-ppt-19-320.jpg)


![HIGH ALTITUDE SICKNESS 3[1].ppt](https://image.slidesharecdn.com/highaltitudesickness31-230905155430-23668e28/85/HIGH-ALTITUDE-SICKNESS-3-1-ppt-23-320.jpg)
![HIGH ALTITUDE SICKNESS 3[1].ppt](https://image.slidesharecdn.com/highaltitudesickness31-230905155430-23668e28/85/HIGH-ALTITUDE-SICKNESS-3-1-ppt-24-320.jpg)
![HIGH ALTITUDE SICKNESS 3[1].ppt](https://image.slidesharecdn.com/highaltitudesickness31-230905155430-23668e28/85/HIGH-ALTITUDE-SICKNESS-3-1-ppt-25-320.jpg)


HIGH ALTITUDE SICKNESS 3[1].ppt
- 1. HIGH ALTITUDE MEDICAL DISORDERS (AHAI) DR MOHD YOUSUF
- 3. Purpose of going to high altitude Amaranth cave 5486 m
- 5. Men at work
- 6. Phase 2 Gandola Height 4200 m
- 7. REFERENCE CASE ŌĆó A 25 year old male was brought to AE with complaints of sudden onset Shortness of breath and Headache which developed 16 hours after ascending to 2nd Phase of Afarvat peak Gulmarg via cable Car( Gondola)
- 8. ABCDE APPROACHŌĆ”ŌĆ”.. ŌĆó AIRWAYS : PT TALKING ŌĆó BREATHING : RR: 36B/M, SPO2 : 60% on RA, No Abnormal Chest Movements , Equal on both sides , B/L crepts .No murmur ŌĆó CIRCULATION : HR : 120 B/M BP 120/80, CRT ; 2 secs, Warm and Pink extremities. ŌĆó DISABLITY : AVPU : ALERT, RESTLESS, Normal blood glucose , no ABM, Normal Pupil, Normal Muscle Strength, Sensation, Reflexes. ŌĆó Exposure: No External Injuries , Normal Temperature, No Needle Prick, No Rash/Hives.
- 9. SAMPLE HISTORYŌĆ”ŌĆ”ŌĆ”.. ŌĆó SIGNS AND SYMPTOMS : SOB with headache developed after 16 hours of ascend to high alttitude. ŌĆó ALLERGIES : Not significant ŌĆó MEDICATION : No prophylactic medication taken. ŌĆó PAST MEDICAL ILLNESS : No basline comorbidities except smoker ŌĆó LAST MEAL TAKEN : RECENT INTAKE OF ALCOHOL. ŌĆó EVENTS SURROUNDING : low lander from Maharashtra, no previous high altitude travel
- 10. MANAGEMENT; ŌĆó Oxygen via face mask at 6l/min. ŌĆó Paracetamol and Nifedipine 30 mg BD ŌĆó Improved over 4 days and discharged home in stable condition.
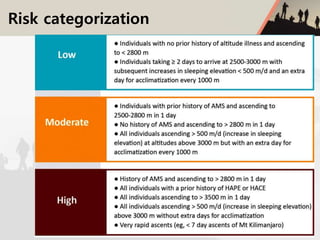
- 13. HIGH ALTITUDE CEREBRAL OEDEMA(HACO) 03 ACUTE MOUNTAIN SICKESS(AMS) 01 HIGH ALTITUDE PULMONARY OEDEMA(HAPO) 02 CHORONIC MORNING SICKNESS(MONGES DISEASE) 04 HIGH ALTITUDE PULMONARY HYPERTENSION 05
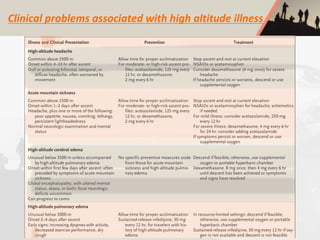
- 14. Clinical problems associated with high altitude illness
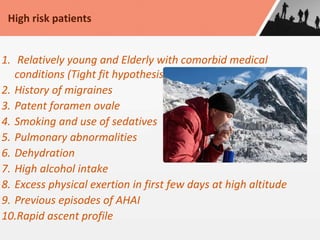
- 16. 1. Relatively young and Elderly with comorbid medical conditions (Tight fit hypothesis) 2. History of migraines 3. Patent foramen ovale 4. Smoking and use of sedatives 5. Pulmonary abnormalities 6. Dehydration 7. High alcohol intake 8. Excess physical exertion in first few days at high altitude 9. Previous episodes of AHAI 10.Rapid ascent profile High risk patients
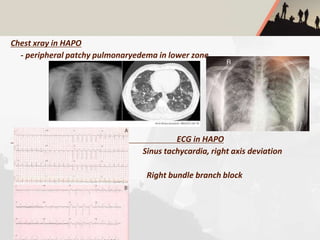
- 17. Chest xray in HAPO - peripheral patchy pulmonaryedema in lower zone ECG in HAPO Sinus tachycardia, right axis deviation Right bundle branch block
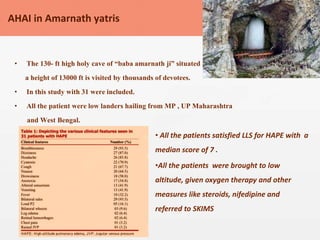
- 21. ŌĆó The 130- ft high holy cave of ŌĆ£baba amarnath jiŌĆØ situated at a height of 13000 ft is visited by thousands of devotees. ŌĆó In this study with 31 were included. ŌĆó All the patient were low landers hailing from MP , UP Maharashtra and West Bengal. AHAI in Amarnath yatris ŌĆó All the patients satisfied LLS for HAPE with a median score of 7 . ŌĆóAll the patients were brought to low altitude, given oxygen therapy and other measures like steroids, nifedipine and referred to SKIMS
- 22. ŌĆó AHAI can be prevented by GRADUAL DESCENT/STAGED DESCENTto promote acclimatisation but yatris ascent rapidly > 600 m /day above 2500 m ŌĆó Identifying people at high risk and giving preventive strategies would be helpful in reducing AMS. ŌĆó Hence providing education and preventive measures is important
- 26. ŌĆó All high altitude travelers,regardless of their underlying health ,are at risk for these problems and should receive counselling regarding recognition, prevention and treatment ŌĆó High altitude headache and AMS are most common ,with the former noted in 37% ascending to 4559 m and latter in 25-40% travelling at 2000-4500 m depending upon the altitude attained and rate of ascent. ŌĆó Although HAPE and HAPO incidents are quite low but are potentially fatal ŌĆó Staged ascent and Ascend high Sleep low. ŌĆó More specifically,once above 3000 m ,travelers should not increase their sleeping elevation by more than 500m per night and including rest day after 2-3 days of ascent. ŌĆó Spending time at intermediate altitudes before ascending to target elevation is called staged ascent ŌĆó Pharmacolgic prophylaxis is not for all but reserved for high risk patients ŌĆó Pretravel evaluation for persons with medical conditions is a must. Advice for all the high altitude travelers (NEJM JAN 2022)
- 28. Replace with your own text Add some text to the title slide THANK YOU