Hiv & leprosy FRIEND OR FOE
Download as pptx, pdf2 likes123 views
This case report describes a 52-year-old male patient with both HIV and leprosy. After starting antiretroviral therapy (ART), the patient developed immune reconstitution inflammatory syndrome (IRIS), with worsening of leprosy symptoms. He was later diagnosed with Dapsone hypersensitivity syndrome after developing a rash and other symptoms while taking Dapsone to treat his leprosy. The report concludes that while HIV and leprosy co-infection can allow immune recovery through IRIS, the patient was at higher risk for adverse cutaneous drug reactions due to HIV, as seen with his reaction to Dapsone.
1 of 29
Download to read offline






Ad
Recommended
Chronic Meningitis Dr. Shatdal Chaudhary
Chronic Meningitis Dr. Shatdal ChaudharyShatdal Chaudhary
╠²
This document discusses chronic meningitis, including its definition, categories, causes, symptoms, diagnostic tests, and treatment. Chronic meningitis is defined as inflammation of the meninges lasting 4 or more weeks, and can be caused by infections, malignancies, or non-infectious inflammatory disorders. Common symptoms are nonspecific but related to anatomical location of inflammation. Diagnosis involves CSF analysis showing characteristics related to possible causes, along with serum tests, imaging, and biopsy if needed. Treatment depends on the identified etiological agent or involves empiric therapy.Aids approach patients
Aids approach patientsMohd Hanafi
╠²
This document discusses Acquired Immunodeficiency Syndrome (AIDS) and Human Immunodeficiency Virus (HIV). It describes how HIV attacks and destroys the immune system, leading to AIDS. It outlines the stages of HIV infection from initial infection through asymptomatic infection to AIDS. It details many opportunistic infections and conditions that can occur in AIDS patients as a result of their weakened immune systems, such as Pneumocystis pneumonia, toxoplasmosis, cryptococcal meningitis, and Kaposi's sarcoma. It also discusses how antiretroviral therapy and prophylaxis can slow progression to AIDS and prevent opportunistic infections.IriS
IriSRajesh Mandal
╠²
Immune Reconstitution Inflammatory Syndrome (IRIS) is a collection of inflammatory disorders associated with paradoxical worsening of preexisting infectious processes following initiation of antiretroviral therapy (ART) in HIV-infected individuals. IRIS occurs in 10-30% of patients starting ART, usually within the first 4-8 weeks. It is more common in patients starting ART with CD4 counts <50 cells/╬╝l. Common pathogens that cause IRIS include Mycobacterium tuberculosis, Cryptococcus, and cytomegalovirus. Symptoms include fever, lymphadenitis, and worsening of pulmonary and neurological symptoms. Management involves continuing ART and treating any underlying infections, with corticosteroidsBacterial meningitis and meningococcal septicaemia
Bacterial meningitis and meningococcal septicaemiaCENTRO MEDICO HUMBOLDT
╠²
The document provides guidance for the management of bacterial meningitis and meningococcal septicaemia in children and young people under 16 in primary and secondary care settings in the UK. It includes recommendations on initial symptoms and assessment, pre-hospital management, diagnosis, treatment and long-term management. The guidance aims to optimize care for this patient population while respecting patient preferences and the need for informed consent.Early recognition of meningitis
Early recognition of meningitisMeningitis Research Foundation
╠²
The document discusses guidelines for the recognition and management of bacterial meningitis and meningococcal septicaemia in children and young people, emphasizing the importance of early diagnosis and training for healthcare professionals. It highlights common misdiagnoses, signs of severe disease, and the critical need for prompt referral and intervention. Additionally, it outlines follow-up care and the potential long-term effects of the disease on patients.20160720 Japanese encephalitis
20160720 Japanese encephalitisJin-Yi Hsu
╠²
This document discusses two cases of Japanese encephalitis in patients, highlighting clinical findings such as MRI results, blood tests, and neurological symptoms. The final diagnosis for both patients included encephalitis with lesions in critical brain areas, as well as complications like hepatic and renal impairment. It also addresses differential diagnosis, treatment options, and potential long-term prognostic factors based on past clinical data.Fever
FeverProf. Dr. Aswinikumar Surendran
╠²
A patient presenting with acute febrile illness should be treated with consideration and caution. Most cases will resolve without complication, but identifying the small percentage with potential life-threatening conditions requires careful examination and investigation over time. Making an early diagnosis risks missing unexpected developments, so empirical treatment should not be withheld in severe situations while the illness course is monitored.Immunodeficiency in children 2015
Immunodeficiency in children 2015Azad Haleem
╠²
This document outlines immunology and immunity to infection. It discusses the immune system's role in fighting infection, including humoral immunity from B cells and cellular immunity from T cells. It also addresses intracellular and extracellular pathogens. The document then focuses on primary and secondary immunodeficiency, describing the types of primary immunodeficiencies including B cell, T cell, phagocytic, and complement defects. It provides guidance on diagnosing immunodeficiency through history, examination, investigations, and considering features like recurrent infections.Viral heamorraghic fever
Viral heamorraghic fever mohammedlukman
╠²
This document provides an overview of viral hemorrhagic fever (VHF) and focuses on yellow fever. It classifies VHFs and describes their pathogenesis. Yellow fever is caused by a flavivirus transmitted by mosquitoes. It presents with fever, bleeding, liver and kidney damage. Diagnosis involves blood tests showing low platelets and clotting factors. Treatment focuses on supportive care; vaccines can prevent yellow fever.Immune reconstitution inflammatory syndrome-Hamisi Mkindi
Immune reconstitution inflammatory syndrome-Hamisi MkindiMkindi Mkindi
╠²
Immune reconstitution inflammatory syndrome (IRIS) occurs in some AIDS or immunosuppressed patients when the immune system recovers, resulting in an exaggerated inflammatory response to opportunistic infections. Risk factors include low CD4 counts and rapid initiation of antiretroviral therapy (ART). Diagnosis involves atypical presentations of infections, elevation in CD4 counts, and spontaneous symptom resolution, with management focusing on monitoring, corticosteroids, and patient education on the risks associated with ART.Non resolving pneumonia
Non resolving pneumoniaDr. RAJKOTI REDDY GONDI
╠²
1. Dr. Rajkoti discusses the approach to evaluating and managing non-resolving pneumonia. Key factors that can delay resolution are host factors like age, comorbidities, and smoking as well as drug-resistant or unusual pathogens.
2. Three case studies are presented. The first involves a teenage boy with empyema that required drainage. The second is a middle-aged man with hypersensitivity pneumonitis related to his job that responded to steroids. The third involves further evaluation of a woman's non-productive cough to identify potential non-infectious causes.
3. For non-resolving pneumonia, re-emphasis is placed on thorough history, microbiology testing, imaging,Immunodeficiency disorders,2010
Immunodeficiency disorders,2010ž»┘āž¬┘łž▒ ┘ģž▒┘ŖžČ
╠²
Immunodeficiency disorders are associated with defects or impairments in immune function that can be congenital or acquired. Primary immunodeficiency diseases involve genetic defects affecting B cell, T cell, or phagocytic cell development. Common symptoms include recurrent infections, failure to thrive, and increased susceptibility to opportunistic infections. HIV/AIDS is an acquired immunodeficiency disorder that progressively weakens the immune system by attacking CD4 cells, leaving the body vulnerable to opportunistic infections.Puo
Puomandar haval
╠²
This document discusses pyrexia of unknown origin (PUO), defined as a fever without an obvious source based on clinical examination. It provides details on age groups for PUO, including neonates less than 28 days who should be hospitalized due to high risk of serious bacterial infection. For infants 1-3 months, certain criteria like appearance, white blood cell count and urine analysis determine if further investigation and treatment is needed. Causes of PUO are discussed, with the most common being a common disease presenting atypically. Management involves investigation and potential antibiotic treatment depending on age and symptoms.HIV
HIVguestd9420
╠²
The document provides an outline on HIV pathophysiology, epidemiology, clinical manifestations, and treatment. It discusses how HIV causes immunosuppression leading to opportunistic infections affecting the respiratory, cardiac, neurological, ophthalmological, gastrointestinal, and renal systems. Common opportunistic infections include Pneumocystis jirovecii pneumonia, tuberculosis, toxoplasmosis, cryptococcosis, and cytomegalovirus retinitis. Treatment involves antiretroviral therapy and prophylaxis depending on CD4 count. Health care providers need to consider acute HIV infection and opportunistic diseases in patients presenting with related symptoms.Approach to acute febrile illness
Approach to acute febrile illnessFadel Muhammad Garishah
╠²
This document provides guidance on evaluating and managing acute febrile illness in returning travelers. It outlines:
1) Common causes of fever in returning travelers, including malaria, dengue, influenza, and enteric fever.
2) Recommendations for obtaining a thorough travel history, physical exam, and diagnostic testing based on the patient's symptoms, risk factors, and travel destinations.
3) Treatment guidelines for various infections based on disease severity and suspected pathogen.Covid 19 in immunocompromised patients
Covid 19 in immunocompromised patientsFawzia Abo-Ali
╠²
This document discusses COVID-19 in immunocompromised patients. It notes that while immunocompromised patients are at higher risk of severe COVID-19 due to an impaired immune response, the suppression of inflammation may also be protective. The effects of various immunocompromising conditions like HIV, cancer, transplant recipients, and primary immunodeficiencies on COVID-19 outcomes are reviewed. Management strategies like antiviral therapy and immunoglobulin replacement are also discussed. More research is still needed to understand how immunocompromise impacts COVID-19 severity.Influenza antivial medications
Influenza antivial medications Ashraf ElAdawy
╠²
1. Influenza can range from mild to severe illness and sometimes lead to hospitalization or death. Patients at high risk tend to experience more severe illness.
2. Patients with mild influenza typically recover within a week without treatment, while those with severe or complicated cases may need hospitalization and antiviral drugs.
3. Antiviral drugs like oseltamivir work best when given within 48 hours of symptoms but may still provide benefit even after that for severe cases. Clinical judgment is important when deciding on antiviral treatment.Covid 19
Covid 19Ayman Allam
╠²
The document discusses coronaviruses and COVID-19. It notes that coronaviruses can infect humans and cause diseases like the common cold, SARS, and MERS. COVID-19 is caused by a new coronavirus called SARS-CoV-2 that was first detected in Wuhan, China in December 2019 and causes respiratory illness. Symptoms range from mild to severe pneumonia and death. While there is no vaccine yet, prevention focuses on hand washing, social distancing, and isolation of sick individuals.Clinial Manifestations of Dengue Fever
Clinial Manifestations of Dengue FeverProf. Dr. Aswinikumar Surendran
╠²
This document summarizes clinical manifestations of dengue fever, dengue hemorrhagic fever, and dengue shock syndrome. It describes how dengue is caused by a virus transmitted by Aedes mosquitos. It outlines the disease progression from primary to secondary infection and discusses disease definitions. Key points include four clinical syndromes, hemorrhagic manifestations, thrombocytopenia, and signs of circulatory failure in dengue shock syndrome.Covid 19 Presentation and diagnosis
Covid 19 Presentation and diagnosisjamalumar3
╠²
This document provides information on COVID-19 presentation and diagnosis. It discusses how the virus is transmitted via respiratory droplets, its pathogenesis by binding the ACE2 receptor, and typical symptoms like fever, cough and breathlessness. It outlines risk factors for severe disease like older age and comorbidities. Diagnostic tests involve PCR of respiratory samples and chest imaging showing patchy ground glass opacities. Prognosis is poor with increased oxygen needs, lymphopenia and elevated inflammatory markers.Dengue and Dengue Hemorrhagic Fever
Dengue and Dengue Hemorrhagic Fever Jega Subramaniam
╠²
The document provides a comprehensive overview of dengue fever and dengue hemorrhagic fever, detailing the causative virus, epidemiology, clinical manifestations, pathogenesis, diagnosis, and prevention measures. It highlights the crucial role of specific mosquito vectors in transmission and the significant public health burden posed by dengue globally. Additionally, the document outlines diagnostic criteria, treatment options, and case studies to illustrate key concepts related to the disease.Phagocytic dysfunction
Phagocytic dysfunctionMR. JAGDISH SAMBAD
╠²
Phagocytic dysfunction, often genetic, impairs the innate immune system, particularly neutrophils, leading to an inability to respond to infections. Symptoms include increased susceptibility to bacterial, fungal, and viral infections, chronic skin conditions, and oral issues. Management involves early diagnosis, granulocyte transfusions, and treatment with growth factors to boost immune cell production.Acute Rheumatic Fever in children
Acute Rheumatic Fever in childrenGanapathy Tamilselvan
╠²
This document provides an overview of acute rheumatic fever in children. It discusses the definition, risk factors including age and environment, etiology as a post-infection complication of streptococcal tonsillitis or pharyngitis, pathogenesis involving autoimmune response and cross-reactivity, classification, diagnostic criteria, treatment and prophylaxis. Specific syndromes associated with acute rheumatic fever like rheumatic polyarthritis, chorea, rheumatic heart disease, pericarditis and criteria for assessing rheumatic activity are also outlined.Meningitis
MeningitisGaurabPandey2
╠²
Meningitis is the inflammation of the meninges caused primarily by infections from bacteria, viruses, fungi, or parasites. It can lead to severe complications if untreated, such as hearing loss and brain damage, and symptoms vary by age and type; common signs include fever, headache, and neck stiffness. Diagnosis involves a medical history review and tests like lumbar puncture, while treatment options depend on the cause, ranging from antibiotics for bacterial meningitis to supportive care for viral forms.Hiv infections
Hiv infectionsDr. JAKEER HUSSAIN
╠²
HIV infects and destroys CD4 lymphocytes, lowering immunity and allowing opportunistic infections. Various infections are associated with different CD4 count thresholds, including Pneumocystis pneumonia below 200, histoplasmosis below 150, and Mycobacterium avium complex below 50. Tuberculosis co-infection increases HIV risk and disease progression. Common opportunistic infections include Pneumocystis pneumonia, bacterial pneumonia, cryptococcal meningitis, toxoplasmosis, and disseminated Mycobacterium. Diagnosis and treatment depends on the specific infection.HIV IN PEDIATRIC DENTISTRY
HIV IN PEDIATRIC DENTISTRYSohail Mohammed
╠²
HIV can infect children perinatally or during birth. It attacks CD4 cells and progresses through acute infection, asymptomatic infection, and AIDS stages as CD4 counts fall. Common symptoms in children include failure to thrive, recurrent infections, and developmental delays. Respiratory infections like pneumonia are major causes of illness. Diagnosis involves clinical evaluation and CD4 counts. Treatment aims to suppress viral loads and treat opportunistic infections.Diseases
DiseasesHawkesdale P12 College
╠²
This document provides an overview of different types of diseases including infectious, non-infectious, nutritional, genetic, cancers, auto-immune, and those caused by pathogens. Infectious diseases are caused by pathogens like viruses, bacteria, fungi, parasites, or prions. Non-infectious diseases have other causes like poor nutrition, smoking, pollution, and genetics. Examples of specific nutritional deficiency diseases, genetic diseases, cancers, and auto-immune diseases are also outlined. The document concludes by describing different pathogens and vectors that can transmit diseases.Meningitis
Meningitisroshnee khadka
╠²
This document discusses meningitis, including its causes, types, symptoms, diagnosis, and treatment. Meningitis is an inflammation of the meninges, which are the protective membranes surrounding the brain and spinal cord. It can be caused by bacterial, viral, or fungal infections. Bacterial meningitis requires urgent treatment with antibiotics as it can be life-threatening. Symptoms vary depending on age but may include fever, headache, stiff neck, nausea, confusion, and seizures. Diagnosis involves physical exam, spinal fluid analysis, and imaging tests. Treatment focuses on identifying the cause, administering antibiotics or antivirals, relieving symptoms, and preventing complications.Dermatology in HIV
Dermatology in HIVDr Yugandar
╠²
This study examined 110 known HIV-positive patients with skin lesions in Central India over 2 years. 53 patients (48%) had infectious skin pathology including viral (27.28%), bacterial (12.72%), fungal (5.45%), and parasitic (6.36%) infections. The most common were molluscum contagiosum and HPV lesions. 37 patients (35%) had non-infectious pathology such as pruritic papular eruptions. Infectious lesions were more common in patients with CD4 counts below 350, while non-infectious lesions were more common above 350. Unusual presentations of infectious agents were observed in 57 patients (52%). Cutaneous manifestations can serve as early indicatorsTypical and atypical manifestations of leprosy
Typical and atypical manifestations of leprosyChetan Ganteppanavar
╠²
This document discusses leprosy, including its definition, etiology, classification, clinical manifestations, diagnosis, and treatment. It defines leprosy as a chronic disease caused by Mycobacterium leprae that affects the skin and nerves. Leprosy is classified into several types depending on clinical features and bacterial load. Diagnosis involves skin smears, biopsy, and nerve conduction studies. Treatment involves multidrug therapy and steroids for leprosy reactions.More Related Content
What's hot (20)
Viral heamorraghic fever
Viral heamorraghic fever mohammedlukman
╠²
This document provides an overview of viral hemorrhagic fever (VHF) and focuses on yellow fever. It classifies VHFs and describes their pathogenesis. Yellow fever is caused by a flavivirus transmitted by mosquitoes. It presents with fever, bleeding, liver and kidney damage. Diagnosis involves blood tests showing low platelets and clotting factors. Treatment focuses on supportive care; vaccines can prevent yellow fever.Immune reconstitution inflammatory syndrome-Hamisi Mkindi
Immune reconstitution inflammatory syndrome-Hamisi MkindiMkindi Mkindi
╠²
Immune reconstitution inflammatory syndrome (IRIS) occurs in some AIDS or immunosuppressed patients when the immune system recovers, resulting in an exaggerated inflammatory response to opportunistic infections. Risk factors include low CD4 counts and rapid initiation of antiretroviral therapy (ART). Diagnosis involves atypical presentations of infections, elevation in CD4 counts, and spontaneous symptom resolution, with management focusing on monitoring, corticosteroids, and patient education on the risks associated with ART.Non resolving pneumonia
Non resolving pneumoniaDr. RAJKOTI REDDY GONDI
╠²
1. Dr. Rajkoti discusses the approach to evaluating and managing non-resolving pneumonia. Key factors that can delay resolution are host factors like age, comorbidities, and smoking as well as drug-resistant or unusual pathogens.
2. Three case studies are presented. The first involves a teenage boy with empyema that required drainage. The second is a middle-aged man with hypersensitivity pneumonitis related to his job that responded to steroids. The third involves further evaluation of a woman's non-productive cough to identify potential non-infectious causes.
3. For non-resolving pneumonia, re-emphasis is placed on thorough history, microbiology testing, imaging,Immunodeficiency disorders,2010
Immunodeficiency disorders,2010ž»┘āž¬┘łž▒ ┘ģž▒┘ŖžČ
╠²
Immunodeficiency disorders are associated with defects or impairments in immune function that can be congenital or acquired. Primary immunodeficiency diseases involve genetic defects affecting B cell, T cell, or phagocytic cell development. Common symptoms include recurrent infections, failure to thrive, and increased susceptibility to opportunistic infections. HIV/AIDS is an acquired immunodeficiency disorder that progressively weakens the immune system by attacking CD4 cells, leaving the body vulnerable to opportunistic infections.Puo
Puomandar haval
╠²
This document discusses pyrexia of unknown origin (PUO), defined as a fever without an obvious source based on clinical examination. It provides details on age groups for PUO, including neonates less than 28 days who should be hospitalized due to high risk of serious bacterial infection. For infants 1-3 months, certain criteria like appearance, white blood cell count and urine analysis determine if further investigation and treatment is needed. Causes of PUO are discussed, with the most common being a common disease presenting atypically. Management involves investigation and potential antibiotic treatment depending on age and symptoms.HIV
HIVguestd9420
╠²
The document provides an outline on HIV pathophysiology, epidemiology, clinical manifestations, and treatment. It discusses how HIV causes immunosuppression leading to opportunistic infections affecting the respiratory, cardiac, neurological, ophthalmological, gastrointestinal, and renal systems. Common opportunistic infections include Pneumocystis jirovecii pneumonia, tuberculosis, toxoplasmosis, cryptococcosis, and cytomegalovirus retinitis. Treatment involves antiretroviral therapy and prophylaxis depending on CD4 count. Health care providers need to consider acute HIV infection and opportunistic diseases in patients presenting with related symptoms.Approach to acute febrile illness
Approach to acute febrile illnessFadel Muhammad Garishah
╠²
This document provides guidance on evaluating and managing acute febrile illness in returning travelers. It outlines:
1) Common causes of fever in returning travelers, including malaria, dengue, influenza, and enteric fever.
2) Recommendations for obtaining a thorough travel history, physical exam, and diagnostic testing based on the patient's symptoms, risk factors, and travel destinations.
3) Treatment guidelines for various infections based on disease severity and suspected pathogen.Covid 19 in immunocompromised patients
Covid 19 in immunocompromised patientsFawzia Abo-Ali
╠²
This document discusses COVID-19 in immunocompromised patients. It notes that while immunocompromised patients are at higher risk of severe COVID-19 due to an impaired immune response, the suppression of inflammation may also be protective. The effects of various immunocompromising conditions like HIV, cancer, transplant recipients, and primary immunodeficiencies on COVID-19 outcomes are reviewed. Management strategies like antiviral therapy and immunoglobulin replacement are also discussed. More research is still needed to understand how immunocompromise impacts COVID-19 severity.Influenza antivial medications
Influenza antivial medications Ashraf ElAdawy
╠²
1. Influenza can range from mild to severe illness and sometimes lead to hospitalization or death. Patients at high risk tend to experience more severe illness.
2. Patients with mild influenza typically recover within a week without treatment, while those with severe or complicated cases may need hospitalization and antiviral drugs.
3. Antiviral drugs like oseltamivir work best when given within 48 hours of symptoms but may still provide benefit even after that for severe cases. Clinical judgment is important when deciding on antiviral treatment.Covid 19
Covid 19Ayman Allam
╠²
The document discusses coronaviruses and COVID-19. It notes that coronaviruses can infect humans and cause diseases like the common cold, SARS, and MERS. COVID-19 is caused by a new coronavirus called SARS-CoV-2 that was first detected in Wuhan, China in December 2019 and causes respiratory illness. Symptoms range from mild to severe pneumonia and death. While there is no vaccine yet, prevention focuses on hand washing, social distancing, and isolation of sick individuals.Clinial Manifestations of Dengue Fever
Clinial Manifestations of Dengue FeverProf. Dr. Aswinikumar Surendran
╠²
This document summarizes clinical manifestations of dengue fever, dengue hemorrhagic fever, and dengue shock syndrome. It describes how dengue is caused by a virus transmitted by Aedes mosquitos. It outlines the disease progression from primary to secondary infection and discusses disease definitions. Key points include four clinical syndromes, hemorrhagic manifestations, thrombocytopenia, and signs of circulatory failure in dengue shock syndrome.Covid 19 Presentation and diagnosis
Covid 19 Presentation and diagnosisjamalumar3
╠²
This document provides information on COVID-19 presentation and diagnosis. It discusses how the virus is transmitted via respiratory droplets, its pathogenesis by binding the ACE2 receptor, and typical symptoms like fever, cough and breathlessness. It outlines risk factors for severe disease like older age and comorbidities. Diagnostic tests involve PCR of respiratory samples and chest imaging showing patchy ground glass opacities. Prognosis is poor with increased oxygen needs, lymphopenia and elevated inflammatory markers.Dengue and Dengue Hemorrhagic Fever
Dengue and Dengue Hemorrhagic Fever Jega Subramaniam
╠²
The document provides a comprehensive overview of dengue fever and dengue hemorrhagic fever, detailing the causative virus, epidemiology, clinical manifestations, pathogenesis, diagnosis, and prevention measures. It highlights the crucial role of specific mosquito vectors in transmission and the significant public health burden posed by dengue globally. Additionally, the document outlines diagnostic criteria, treatment options, and case studies to illustrate key concepts related to the disease.Phagocytic dysfunction
Phagocytic dysfunctionMR. JAGDISH SAMBAD
╠²
Phagocytic dysfunction, often genetic, impairs the innate immune system, particularly neutrophils, leading to an inability to respond to infections. Symptoms include increased susceptibility to bacterial, fungal, and viral infections, chronic skin conditions, and oral issues. Management involves early diagnosis, granulocyte transfusions, and treatment with growth factors to boost immune cell production.Acute Rheumatic Fever in children
Acute Rheumatic Fever in childrenGanapathy Tamilselvan
╠²
This document provides an overview of acute rheumatic fever in children. It discusses the definition, risk factors including age and environment, etiology as a post-infection complication of streptococcal tonsillitis or pharyngitis, pathogenesis involving autoimmune response and cross-reactivity, classification, diagnostic criteria, treatment and prophylaxis. Specific syndromes associated with acute rheumatic fever like rheumatic polyarthritis, chorea, rheumatic heart disease, pericarditis and criteria for assessing rheumatic activity are also outlined.Meningitis
MeningitisGaurabPandey2
╠²
Meningitis is the inflammation of the meninges caused primarily by infections from bacteria, viruses, fungi, or parasites. It can lead to severe complications if untreated, such as hearing loss and brain damage, and symptoms vary by age and type; common signs include fever, headache, and neck stiffness. Diagnosis involves a medical history review and tests like lumbar puncture, while treatment options depend on the cause, ranging from antibiotics for bacterial meningitis to supportive care for viral forms.Hiv infections
Hiv infectionsDr. JAKEER HUSSAIN
╠²
HIV infects and destroys CD4 lymphocytes, lowering immunity and allowing opportunistic infections. Various infections are associated with different CD4 count thresholds, including Pneumocystis pneumonia below 200, histoplasmosis below 150, and Mycobacterium avium complex below 50. Tuberculosis co-infection increases HIV risk and disease progression. Common opportunistic infections include Pneumocystis pneumonia, bacterial pneumonia, cryptococcal meningitis, toxoplasmosis, and disseminated Mycobacterium. Diagnosis and treatment depends on the specific infection.HIV IN PEDIATRIC DENTISTRY
HIV IN PEDIATRIC DENTISTRYSohail Mohammed
╠²
HIV can infect children perinatally or during birth. It attacks CD4 cells and progresses through acute infection, asymptomatic infection, and AIDS stages as CD4 counts fall. Common symptoms in children include failure to thrive, recurrent infections, and developmental delays. Respiratory infections like pneumonia are major causes of illness. Diagnosis involves clinical evaluation and CD4 counts. Treatment aims to suppress viral loads and treat opportunistic infections.Diseases
DiseasesHawkesdale P12 College
╠²
This document provides an overview of different types of diseases including infectious, non-infectious, nutritional, genetic, cancers, auto-immune, and those caused by pathogens. Infectious diseases are caused by pathogens like viruses, bacteria, fungi, parasites, or prions. Non-infectious diseases have other causes like poor nutrition, smoking, pollution, and genetics. Examples of specific nutritional deficiency diseases, genetic diseases, cancers, and auto-immune diseases are also outlined. The document concludes by describing different pathogens and vectors that can transmit diseases.Meningitis
Meningitisroshnee khadka
╠²
This document discusses meningitis, including its causes, types, symptoms, diagnosis, and treatment. Meningitis is an inflammation of the meninges, which are the protective membranes surrounding the brain and spinal cord. It can be caused by bacterial, viral, or fungal infections. Bacterial meningitis requires urgent treatment with antibiotics as it can be life-threatening. Symptoms vary depending on age but may include fever, headache, stiff neck, nausea, confusion, and seizures. Diagnosis involves physical exam, spinal fluid analysis, and imaging tests. Treatment focuses on identifying the cause, administering antibiotics or antivirals, relieving symptoms, and preventing complications.Similar to Hiv & leprosy FRIEND OR FOE (20)
Dermatology in HIV
Dermatology in HIVDr Yugandar
╠²
This study examined 110 known HIV-positive patients with skin lesions in Central India over 2 years. 53 patients (48%) had infectious skin pathology including viral (27.28%), bacterial (12.72%), fungal (5.45%), and parasitic (6.36%) infections. The most common were molluscum contagiosum and HPV lesions. 37 patients (35%) had non-infectious pathology such as pruritic papular eruptions. Infectious lesions were more common in patients with CD4 counts below 350, while non-infectious lesions were more common above 350. Unusual presentations of infectious agents were observed in 57 patients (52%). Cutaneous manifestations can serve as early indicatorsTypical and atypical manifestations of leprosy
Typical and atypical manifestations of leprosyChetan Ganteppanavar
╠²
This document discusses leprosy, including its definition, etiology, classification, clinical manifestations, diagnosis, and treatment. It defines leprosy as a chronic disease caused by Mycobacterium leprae that affects the skin and nerves. Leprosy is classified into several types depending on clinical features and bacterial load. Diagnosis involves skin smears, biopsy, and nerve conduction studies. Treatment involves multidrug therapy and steroids for leprosy reactions.Mycobacterium leprae
Mycobacterium lepraeDeepak Chaudhary
╠²
This document provides information about leprosy (Hansen's disease), including:
- It is caused by Mycobacterium leprae and primarily affects the skin, nerves, and mucosa.
- There are several classification systems including paucibacillary, multibacillary, lepromatous, tuberculoid, and borderline. Classification depends on immune response and bacterial load.
- It remains a major public health problem with millions of cases worldwide, especially in India, Brazil, and African countries. Treatment involves multidrug therapy to prevent disability.Leprosy microbiology
Leprosy microbiologySaachiGupta4
╠²
Leprosy, caused by Mycobacterium leprae, is a chronic bacterial disease recognized since ancient times, first identified by Hansen in 1873. It manifests in various forms, primarily lepromatous and tuberculoid, distinguished by skin lesions and immune response; treatment options vary based on bacillary load. Early diagnosis through laboratory techniques and careful management can prevent severe complications and deformities in affected individuals.Cutaneous manifestations of HIV
Cutaneous manifestations of HIVYugandhar Tummala
╠²
Cutaneous manifestations are common in patients with HIV/AIDS and can present as the earliest sign of infection. A wide variety of bacterial, viral, fungal and parasitic infections can affect the skin, such as herpes simplex virus, varicella zoster virus, human papilloma virus, and molluscum contagiosum virus. Non-infectious conditions like Kaposi's sarcoma and seborrheic dermatitis are also more prevalent. Recognition of cutaneous signs is important for early diagnosis and treatment of HIV, as skin disorders can severely impact quality of life.Leprosy
LeprosyGSL medical college
╠²
Leprosy is a chronic infectious disease caused by Mycobacterium leprae. It primarily affects the skin and peripheral nerves. Left untreated, it can cause permanent damage to the skin, nerves, limbs, and eyes. It is classified clinically into three main types based on immunity - indeterminate leprosy, borderline tuberculoid leprosy, and borderline lepromatous leprosy. Treatment involves multidrug therapy with dapsone, clofazimine, rifampin and ofloxacin to kill the bacteria and prevent further nerve damage and disability. Reactions during treatment called lepra reactions can cause worsening of symptoms and are managed with anti-inflammatory drugs. PreventionLeprosy & Syphilis
Leprosy & SyphilisDr. Varughese George
╠²
This document provides information about leprosy (Hansen's disease):
1. Leprosy is a chronic infectious disease caused by Mycobacterium leprae that affects the peripheral nerves, skin, and mucous membranes.
2. Symptoms can develop slowly over many years and result in skin lesions and deformities of the hands, feet, eyes, and ears.
3. Leprosy exists on a spectrum from tuberculoid to lepromatous forms depending on the immune response; it is diagnosed based on clinical features and confirmation with skin smears or biopsy.12HIV.ppt
12HIV.pptHussen39
╠²
This document discusses the various skin manifestations that can occur in patients with HIV/AIDS. It notes that up to 92% of patients will experience one or more skin disorders throughout their illness. Conditions range from common issues like seborrheic dermatitis and xerosis to more specific diseases such as Kaposi's sarcoma, bacillary angiomatosis, and oral hairy leukoplakia. Bacterial, viral, and fungal infections are also more frequent and severe in immunocompromised HIV/AIDS patients. Recognizing cutaneous signs of HIV can lead to earlier diagnosis and treatment.HIV-TB Coinfection | Jindal chest clinic
HIV-TB Coinfection | Jindal chest clinicJindal Chest Clinic
╠²
The document discusses the complexities of tuberculosis (TB) co-infection with HIV, highlighting the increasing incidence of TB in relation to the HIV epidemic, especially in Africa and India. It outlines the clinical manifestations, challenges in diagnosis, and treatment protocols, emphasizing the importance of managing both infections concurrently and addressing drug interactions. The findings suggest that without effective management and treatment, the burden of TB among HIV-positive populations will significantly worsen.Leprosy
LeprosyDr Subodh Shah
╠²
This document discusses leprosy (Hansen's disease), caused by Mycobacterium leprae bacteria. It describes the classification systems for leprosy, including Ridley-Jopling and paucibacillary vs multibacillary. The typical skin lesions, nerve involvement, and systemic manifestations are outlined for each type of leprosy. Diagnosis involves identification of cardinal signs on skin or nerves, skin smears, and biopsy. Treatment involves multidrug therapy to prevent disability, while general measures focus on education, wound care, and counseling for treatment adherence. Untreated leprosy can cause permanent damage such as disfigurement, hair loss, muscle weakness, nerve damage, and eye complications.Mycobacteria
MycobacteriaTONY SCARIA
╠²
- Atypical mycobacteria include nontuberculous mycobacteria found in the environment that can cause disease in humans under certain conditions.
- Mycobacterium leprae causes leprosy (Hansen's disease), with a spectrum of clinical manifestations depending on immune response from tuberculoid to lepromatous leprosy.
- Diagnosis involves skin smears and biopsy showing acid-fast bacilli. Treatment is multidrug therapy including dapsone, rifampin, and clofazimine.leprosy final.pptx
leprosy final.pptxShubham Shukla
╠²
This document provides an overview of leprosy (Hansen's disease). It discusses the history, epidemiology, etiology, classification, pathogenesis, transmission, clinical features, treatment, reactions, and management of leprosy. Leprosy is caused by Mycobacterium leprae and mainly affects the skin and peripheral nerves. It is treated using multidrug therapy regimens as recommended by the WHO. Management involves treatment, prevention of disabilities, and social integration programs.14.HIV and periodontium.pptx
14.HIV and periodontium.pptxDrNavyadidla
╠²
This document discusses HIV/AIDS and its effects on the periodontium. It begins with an overview of HIV, how it is transmitted, and its pathogenesis. It then describes various oral manifestations of HIV infection, including oral candidiasis, hairy leukoplakia, Kaposi's sarcoma, non-Hodgkin's lymphoma, and periodontal diseases. Diagnosis and treatment approaches for each condition are provided. The document emphasizes that proper oral hygiene and treatment can help support periodontal health in HIV-positive individuals.Department of pathology case presentation
Department of pathology case presentationKristine Turqueza
╠²
A 61-year-old male presented with a 2-year history of a tender, erythematous macular skin lesion on his back. Biopsy of the lesion revealed acid-fast bacilli and spindle-shaped cells forming a storiform pattern, consistent with leprosy. Leprosy, also known as Hansen's disease, is caused by Mycobacterium leprae and presents along a clinical spectrum from tuberculoid to lepromatous forms. While treatable with multidrug therapy, leprosy continues to cause disability through inflammatory episodes known as reactions.Hiv
HivNoeleen Bamuza
╠²
This document discusses various dermatological manifestations seen in HIV/AIDS patients. It covers infectious conditions like herpes simplex, varicella zoster, molluscum contagiosum, staphylococcus infections, and fungal infections. It also discusses non-infectious conditions like seborrheic dermatitis and psoriasis. Finally, it covers neoplasms associated with HIV like Kaposi's sarcoma and lymphomas. For each condition, it provides details on clinical features, diagnosis, and treatment recommendations. The document serves as a comprehensive reference for dermatological problems commonly encountered in HIV patients.It is for educational purpose only HIV 2.ppt
It is for educational purpose only HIV 2.pptGETNET WONDIM
╠²
Up to 92% of HIV/AIDS patients experience skin disorders, with unique conditions like bacillary angiomatosis and oral hairy leukoplakia serving as early indicators of the disease. Common skin manifestations include seborrhoeic dermatitis, xerosis, and eosinophilic folliculitis, while severe infections such as bacterial and fungal infections are prevalent in advanced immunodeficiency. The document also highlights the significance of lesions like warts and herpes infections as critical complications of HIV, emphasizing the need for appropriate treatment strategies.Granulomatous diseases of the head & neck
Granulomatous diseases of the head & neckMammootty Ik
╠²
The document provides an overview of granulomatous diseases affecting the head and neck, detailing their etiology, classification, clinical features, diagnosis, and treatment options. It covers specific conditions such as tuberculosis, leprosy, and actinomycosis, highlighting their unique characteristics and management strategies. The document emphasizes the importance of accurate diagnosis and tailored therapeutic approaches to effectively handle these complex inflammatory disorders.Leprosy & syphilis
Leprosy & syphilisDr. Varughese George
╠²
Leprosy is a chronic infectious disease caused by Mycobacterium leprae. It is characterized by lesions of the peripheral nerves, skin, and nasal mucosa. There are different clinical classifications of leprosy based on immune response and bacterial load, ranging from tuberculoid leprosy with few bacteria and strong immune response to lepromatous leprosy with many bacteria and weak immune response. Without treatment, leprosy can cause permanent damage, especially to the hands, feet, and face.Cutaneous hiv
Cutaneous hivDR RML DELHI
╠²
Cutaneous manifestations are common in HIV patients, occurring in over 90% of cases. They can represent the first signs of HIV infection and have prognostic significance. Skin conditions in HIV patients often present atypically with lesions in unusual sites, atypical morphology, being more extensive or not responding to conventional treatments. Common manifestations include generalized rashes, oral/genital ulcers, seborrheic dermatitis, psoriasis, papulopruritic eruptions, eosinophilic folliculitis, granuloma annulare and various infections like herpes, molluscum, Kaposi sarcoma and non-Hodgkin's lymphoma. Dermatologists must have a high index ofAd
Recently uploaded (20)
Unlocking the Potential of Long-Acting PrEP to Halt HIV Transmissions
Unlocking the Potential of Long-Acting PrEP to Halt HIV TransmissionsPVI, PeerView Institute for Medical Education
╠²
Chair, Allison Agwu, MD, ScM, FAAP, FIDSA, discusses HIV in this CME/MOC/NCPD/CPE/AAPA/IPCE activity titled ŌĆ£Unlocking the Potential of Long-Acting PrEP to Halt HIV Transmissions.ŌĆØ For the full presentation, downloadable Practice Aids, and complete CME/MOC/NCPD/CPE/AAPA/IPCE information, and to apply for credit, please visit us at https://bit.ly/40Mr2AC. CME/MOC/NCPD/CPE/AAPA/IPCE credit will be available until June 12, 2026.Clinical Signs Overview: PICCKLE Mnemonic
Clinical Signs Overview: PICCKLE MnemonicDr Aman Suresh Tharayil
╠²
This presentation provides a concise yet comprehensive review of common clinical signs and their diagnostic significance, summarized under the acronym PICCKLE ŌĆō Pallor, Icterus, Clubbing, Cyanosis, Koilonychia, Lymphadenopathy, and Edema. Each condition is defined, followed by key causes, pathophysiology, diagnostic techniques, and clinical relevance. The content is tailored for undergraduate and postgraduate students in medicine and pharmacy, as well as early-career clinicians seeking to reinforce their clinical examination skillsAbnormal Uterine Bleeding and its Management
Abnormal Uterine Bleeding and its ManagementChandrika Kulkarni
╠²
Abnormal Uterine Bleeding and its ManagementMindfull Midwives: MENTAL WELLBEING OF MIDWIVES FOR BETTER FOR RESPECTFUL MAT...
Mindfull Midwives: MENTAL WELLBEING OF MIDWIVES FOR BETTER FOR RESPECTFUL MAT...LaxmiDeshpande6
╠²
Midwifery practioners should be mindful while caring of mother at all stages like antenatal, postnatal ,during delivery , care of baby.How to be and stay healthy: Live Wire Not a Couch Potato
How to be and stay healthy: Live Wire Not a Couch PotatoBiljanaPipovic
╠²
Live Wire, Not a Couch Potato was an engaging international eTwinning project aimed at promoting physical activity among youth by blending creativity, tradition, and competition. Founded by teachers from Serbia and Portugal, with partners from Turkey and Greece, the project encouraged students to explore the importance of staying active through fun and meaningful challenges. Working within their local contexts, students from all four countries participated in physical activities at school and in their communities. They documented their experiences through photos, videos, and written reflections, which they shared on TwinSpace. The project helped transform exercise from a routine task into an enjoyable, culturally rich experience, while fostering teamwork, creativity, and international exchange.JUNE 2025 ONCOLOGY CARTOONS BY DR KANHU CHARAN PATRO
JUNE 2025 ONCOLOGY CARTOONS BY DR KANHU CHARAN PATROKanhu Charan
╠²
JUNE 2025 ONCOLOGY CARTOONS BY DR KANHU CHARAN PATRODrmohamedaslam_resident_copd2025_fm.pptx
Drmohamedaslam_resident_copd2025_fm.pptxAslam
╠²
COPD :LATEST GUIDELINES 2025
REFERENCE: HarrisonŌĆÖs Principles of Internal Medicine
GOLD -2025 Guidelines
It highlights updated diagnostic criteria, pharmacological and non-pharmacological treatment options, and current best practices for resident doctors and healthcare professionals.
Ideal for medical students, residents, and practitioners seeking an up-to-date, evidence-based reference.
¤æē Download, share, and feel free to reach out for related study material!whooping cough community health nursing.
whooping cough community health nursing.ASWIN S
╠²
Whooping cough for BSC 5th sem community health nursing..
This includes
Introduction
Definition
Incidence
Incubation period
Causes
Clinical manifestations
Diagnostic evaluation
Treatment
Prevention
Complications
Of whooping cough....Aspirin powder or Acetyl salicylic acid powder.docx
Aspirin powder or Acetyl salicylic acid powder.docxkopalsharma85
╠²
pharmacy exercise on aspirin powderHEMOLYTIC ANEMIA - thalassemia, AIHA, and NACP
HEMOLYTIC ANEMIA - thalassemia, AIHA, and NACPSSIMS & RC
╠²
Competency based classes for MBBS students.. Winning GAMBITS Against AML: Guidance on Advances & Medical Breakthroughs wit...
Winning GAMBITS Against AML: Guidance on Advances & Medical Breakthroughs wit...PVI, PeerView Institute for Medical Education
╠²
Chair and Presenter, Naval Daver, MD, Jessica K. Altman, MD, and Ghayas Issa, MD, Alice S. Mims, MD, MSCR, discuss acute myeloid leukemia in this CME/MOC/AAPA/IPCE activity titled ŌĆ£Winning GAMBITS Against AML: Guidance on Advances & Medical Breakthroughs with Innovative Targeted Strategies.ŌĆØ For the full presentation, downloadable Practice Aids, and complete CME/MOC/AAPA/IPCE information, and to apply for credit, please visit us at https://bit.ly/42f1QCa. CME/MOC/AAPA/IPCE credit will be available until June 30, 2026.CEREBRAL PALSY - classification, types and Management
CEREBRAL PALSY - classification, types and ManagementSSIMS & RC
╠²
competency based classes for MBBS students.. Tuberculosis burden , case finding tools and management .pptx
Tuberculosis burden , case finding tools and management .pptxDr. Anu Marhatta
╠²
This presentation is for educational purposes only. nanoparticle and liposomes ppt .(NTDS)pdf
nanoparticle and liposomes ppt .(NTDS)pdfsiddhikalbande
╠²
Nanoparticles and liposomes are advanced carriers used for targeted drug delivery.
Nanoparticles enhance drug effectiveness by directing treatment to specific sites.
Liposomes are biocompatible vesicles that enable controlled and sustained drug release.Unlocking the Potential of Long-Acting PrEP to Halt HIV Transmissions
Unlocking the Potential of Long-Acting PrEP to Halt HIV TransmissionsPVI, PeerView Institute for Medical Education
╠²
Winning GAMBITS Against AML: Guidance on Advances & Medical Breakthroughs wit...
Winning GAMBITS Against AML: Guidance on Advances & Medical Breakthroughs wit...PVI, PeerView Institute for Medical Education
╠²
Ad
Hiv & leprosy FRIEND OR FOE
- 1. Dr. R.V.RANADE M.D.-DERMATOLOGY(Bom), D.D.V(BOM-CPS) Prof. & H.O.D. Dept. of DERMATOLOGY, Dr. D.Y.Patil Medical College. Kolhapur
- 2. HIV & Leprosy Friend or Foe
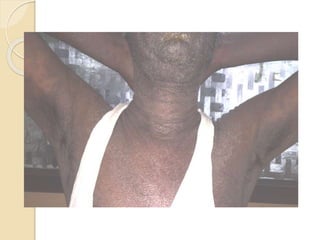
- 3. Case Report ’éŚ VM a 52 years old male admitted in our hospital in first week of July 2015. C/O ’éŚ Fever with chills , high coloured urine- 2 months ’éŚ Swelling around eyes and face-8 days Itching and swelling of face, trunk and extremities-5 days
- 4. ’éŚ Late October2014,patient had fever with chills ,anorexia-18 days ’éŚ At District hospital found to have urinary tract infection ’éŚ H/O Exposure ’éŚ He was HIV +ve and VDRL 1:8 TPHA negative ’éŚ HBs Ag negative ’éŚ CD4 count 297 cells/mm3 ’éŚ Started ART and Co-trimoxazole
- 5. ’éŚ Early March 2015 developed oedematous hypaesthetic plaques on extensor surface of both arms just above elbows. ’éŚ Lt. Ulnar Nerve uniformally thickened, slightly tender ’éŚ Started on MB-MDT and Prednisolone-30 mg tapered to 5 mg OD and then stopped
- 6. ’éŚ End April 2015 he developed fever, icterus and scaling all over body ’éŚ Urine ŌĆōBS, BP PRESENT ’éŚ Total serum Bilirubin-1.31mgs/dl ’éŚ SGPT -119.2 IU/L ’éŚ S. ALKALINE PHOSPATASE- 186 IU/L
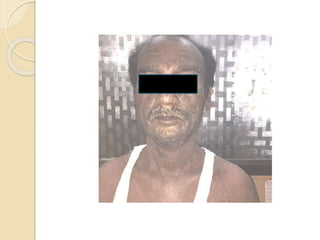
- 7. ’éŚ On admission in our hospital in July 2015 patient had pallor and mild Icterus ’éŚ Oedema of periorbital region ,face and lower limbs ’éŚ Left foot-eczematous crusted plaque ’éŚ Multiple scaly papules and plaques on face trunk and extremities
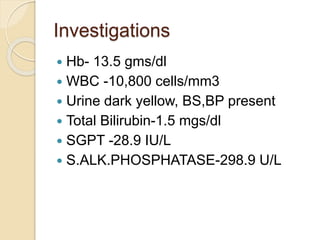
- 12. Investigations ’éŚ Hb- 13.5 gms/dl ’éŚ WBC -10,800 cells/mm3 ’éŚ Urine dark yellow, BS,BP present ’éŚ Total Bilirubin-1.5 mgs/dl ’éŚ SGPT -28.9 IU/L ’éŚ S.ALK.PHOSPHATASE-298.9 U/L
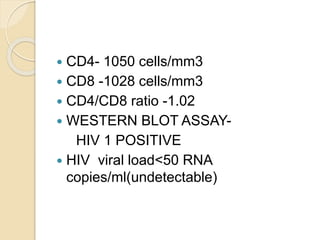
- 13. ’éŚ CD4- 1050 cells/mm3 ’éŚ CD8 -1028 cells/mm3 ’éŚ CD4/CD8 ratio -1.02 ’éŚ WESTERN BLOT ASSAY- HIV 1 POSITIVE ’éŚ HIV viral load<50 RNA copies/ml(undetectable)
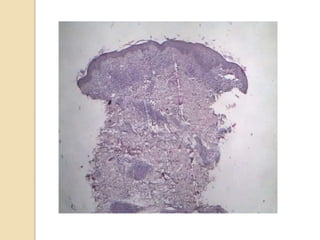
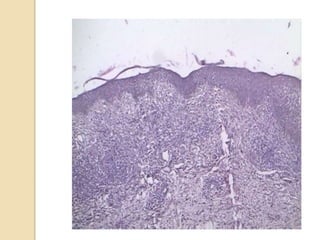
- 16. Biopsy of plaque from left arm ’éŚ Nodular granulomatous inflammation centered around neurovascular bundles ’éŚ Granuloma- lymphocytes epitheloid cells Occasional plasma cells, foreign body and Langhans giant cells ’éŚ Infiltration of dermo-epidermal junction ’éŚ Small amount of lymphocytic nuclear dust suggests Type I reaction. IMPRESSION: BT Hansens with mild type I reaction
- 17. Rx ’éŚ Dapsone and Rifampicin stopped ’éŚ Continued ART ’éŚ Clofazamine, Ofloxacin ’éŚ Methyl prednisolone 16 mg OD tapered to 4 mg OD then stopped
- 18. Present Status ’éŚ During the patientŌĆÖs hospital stay, he had an episode of Herpes progenitalis ’éŚ Treated with Acylovir for 5 days ’éŚ At present the patient has Anorexia,Asthenia and Diarrhoea ŌĆō treated with Cipro + Tinidazole , ’éŚ No fever,itching,oedema ’éŚ Scaling reduced,no icterus ’éŚ Rifampicin has been reinstituted in monthly pulse dosages with Clofazimine and daily Clofazimine and Ofloxacin
- 21. Immune Reconstitution Inflammatory Syndrome (IRIS) ’éŚ Increase in patients lost immune status within 2-4 months of commencing ART (most rapid phase of increased recovery) ’éŚ Incidence 10-20% ’éŚ Sharp increase in CD4 cell count ’éŚ Rx symptomatic- steroids,Thalidomide, Ct ART ’éŚ IRIS unmasks sub clinical infection
- 22. Criteria for diagnosis of IRIS ’éŚ HIV Positive ’éŚ Receiving ART ’éŚ Decrease in HIV-1 RNA level and increase in CD4 + memory cells ’éŚ Clinically inflammatory process ’éŚ Clinical course not consistent with expected results
- 23. IRIS (ctd) ’éŚ IRIS associated with leprosy first described by Lawn et al in 2003 ’éŚ Disease suseptibility gene TNFA- 302*2 for mycobactereal diseases ’éŚ Characterised by development of type I reaction (reversal) in unstable borderline leprosy ’éŚ Low baseline CD4 count -higher risk of IRIS ’éŚ Minimal decrease in viral load in absence of significant increase in CD4 cell count can precipitate IRIS ’éŚ Recognition of Leprosy as an IRIS associate important for timely intervention
- 24. Adverse Cutaneous Drug Reactions (ACDR) ’éŚ Incidence of ACDR high in HIV disease ’éŚ Eruptions more severe than in non-HIV infected ’éŚ Pathogenic mechanisms responsible not known ’éŚ Defects of both T and B cells may be operative in hypersensitivity reactions ’éŚ The patterns of cutaneous reactions may be morbilliform eruptions, FDE,SJS and TEN ’éŚ commonest drugs causing reactions are sulphonamides and penicillins
- 25. Dapsone syndrome ’éŚ Dapsone is a non-antibiotic Sulphonamide(Sulfone) ’éŚ This hypersensitivity is sometimes seen in patients under Rx for some months. ’éŚ Complete form ŌĆōfever, skin rashes- maculopapular type or exfoliative dermatitis with lymphadenopathy and hepatitis usually 4-6 weeks after starting Dapsone ’éŚ In 50% patients one or more manifestations may be missing ’éŚ Dapsone discontinued ’éŚ Short course of steroids and supportive therapy required
- 26. Conclusion ’éŚ Coinfection of HIV with Leprosy is a boon(friend) Patient upgrades immune status(IRIS) ’éŚ In HIV patients, incidence of ACDR high Thus our patient developed Dapsone hypersensitivity syndrome (foe) although prognosis after stopping Dapsone is good. ’éŚ An unusual case of co-existent HIV disease and Leprosy developing first IRIS and then ACDR to Dapsone.