





























IMAGING ANATOMY OF PERITONEAL SPACES.pptx
- 1. IMAGING ANATOMY OF PERITONEAL SPACES Presenter ŌĆō A. Reshmasree Moderator _ DR. Kalaivaani
- 2. PERITONEUM: ŌĆó The peritoneum is a thin, translucent, serous membrane and is the largest and most complexly arranged serous membrane in the body. ŌĆó The peritoneum that lines the abdominal wall is called the parietal peritoneum, whereas the peritoneum that covers a viscus or an organ is called a visceral peritoneum. ŌĆó Both types of peritoneum consist of a single layer of simple low- cuboidal epithelium called a mesothelium. ŌĆó A capillary film of serous fluid (approximately 50ŌĆō100 mL) separates the parietal and visceral layers of peritoneum from one another and lubricates the peritoneal surfaces
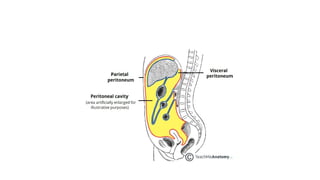
- 3. PERITONEAL CAVITY: ŌĆó The peritoneal cavity is a potential space between the parietal peritoneum, which lines the abdominal wall, and the visceral peritoneum, which envelopes the abdominal organs. ŌĆó In men, the peritoneal cavity is closed. ŌĆó In women, it communicates with the extraperitoneal pelvis exteriorly through the fallopian tubes, uterus and vagina.
- 5. PERITONEAL LIGAMENTS: ŌĆó Peritoneal ligaments are double layers or folds of peritoneum that support a structure within the peritoneal cavity. ŌĆó Omentum: ŌĆó Mesentery or double layer of peritoneum that extends from the stomach and duodenal bulb to adjacent organs. ŌĆó The lesser omentum, which is made of two contiguous components called the gastrohepatic and hepatoduodenal ligaments, attaches the stomach and duodenal bulb to the liver. ŌĆó The greater omentum is attached to the stomach and hangs like an apron from the transverse colon.
- 6. ŌĆó Mesentery : ŌĆó a double layer of peritoneum that encloses an organ and connects it to the abdominal wall. ŌĆó The mesenteric contents include blood vessels, lymph nodes, nerves, and fat. ŌĆó The most mobile parts of the intestine have a mesentery (eg, the small bowel attached to the retroperitoneum), and the retroperitoneal portions of the colon may contain remnant mesocolon, a result of its failure to absorb embryonic mesentery.
- 8. EMBRYOLOGY: ŌĆó The primitive gut forms within the abdominal cavity and is suspended by a plane composed of two peritoneal reflections called the primitive mesenteries, which cover the extension of the subperitoneal space from the abdominal walls. ŌĆó The position of the gut within the primitive mesentery plane divides the primitive mesentery into ventral and dorsal portions, which undergo specialization throughout fetal life.
- 9. ŌĆó Vascular and lymphatic vessels and nerves that supply the abdominal viscera are enfolded within the plane of the primitive mesentery. ŌĆó The liver grows ventral from the gut within the ventral plane. ŌĆó The spleen and pancreas and a major portion of the gut grow within the dorsal plane.
- 12. SUSPENSORY LIGAMENTS OF LIVER ŌĆó Triangular Ligaments. ŌĆó Fusion of peritoneal reflections. ŌĆó The left triangular ligament is formed by the fusion of the inferior and superior reflections of the coronary ligaments. It is short and does not compartmentalize the left subphrenic space. ŌĆó The right triangular ligament is formed by the fusion of the superior and inferior reflections of the right coronary ligament. long and separates the right subphrenic space from the right subhepatic space. ŌĆó The triangular ligaments outline the bare area of the liver
- 13. ŌĆó Falciform Ligament. ŌĆó The remnant of the most ventral part of the ventral mesentery and contains the obliterated umbilical vein. ŌĆó It is a relative (incomplete) barrier to the transfer of fluid from the right subphrenic space to the left subphrenic space.
- 14. Peritoneal Ligaments of the Stomach ŌĆó Lesser Omentum ŌĆó .The gastrohepatic and hepatoduodenal ligaments are contiguous peritoneal ligaments that form the lesser omentum and are remnants of the dorsal portion of the ventral mesentery. ŌĆó The gastrohepatic ligament attaches the lesser curve of the stomach to the liver and contains the coronary vein and left gastric artery ŌĆó The hepatoduodenal ligament attaches the duodenum to the liver and contains the portal vein, hepatic artery, common hepatic ducts, and part of the cystic duct.
- 15. ŌĆó Until the 8th embryonic week, this part of the ventral mesentery also contains the ventral anlage of the pancreas. ŌĆó Hence, the hepatoduodenal ligament is a route of spread of pancreatic disease to the porta hepatis and liver
- 16. ŌĆó Gastrosplenic Ligament. ŌĆó The ventral part of the dorsal mesentery extends between the greater curve of the stomach and the spleen . ŌĆó The superior part of this portion of the dorsal mesentery becomes the gastrosplenic ligament, which contains the short gastric vessels and a collateral route of venous flow after splenic vein thrombosis. ŌĆó The gastrosplenic ligament is a frequent route for subperitoneal spread of pancreatitis-related fluid.
- 18. ŌĆó Greater Omentum. ŌĆó Because of the growth and rotation of the stomach in utero, the inferior aspect of the ventral part of the dorsal mesentery becomes redundant, and its two layers fuse with one another to form the gastrocolic ligament, or the greater omentum. ŌĆó The greater omentum may become visible if it is diseased or if ascites present.
- 20. ŌĆó Splenorenal Ligament. ŌĆó The splenorenal ligament is the most dorsal aspect of the dorsal mesentery. ŌĆó It contains the pancreatic tail and splenorenal collateral vessels in patients with portal hypertension
- 22. Transverse Mesocolon ŌĆó The transverse mesocolon is a peritoneal fold that attaches the transverse colon to the retroperitoneum and contains the middle colic vessels.
- 24. Small Bowel Mesentery ŌĆó The small bowel mesentery attaches the small bowel to the retroperitoneum and extends from the ligament of Treitz to the ileocecal valve. ŌĆó It contains the superior mesenteric vessels and their branches, which mark its position at contrast-enhanced CT. ŌĆó Among the peritoneal structures, the small bowel mesentery is one of the most likely to be involved by metastatic disease. Inflammation and tumor may involve the mesentery directly (eg, from the pancreatic body or jejunum) or by way of the neurovascular plexus or lymphatic channels that run within it.
- 25. Sigmoid Mesocolon ŌĆó The sigmoid mesocolon is a peritoneal ligament that attaches the sigmoid colon to the posterior pelvic wall and contains the hemorrhoidal and sigmoid vessels. ŌĆó The most common pathologic process involving this structure is acute diverticulitis. ŌĆó Perforated cancer and Crohn disease also may cause inflammation within the sigmoid mesocolon.
- 26. Peritoneal spaces ŌĆó The transverse mesocolon divides the peritoneum into the: ŌĆó supramesocolic and inframesocolic spaces ŌĆó paracolic ŌĆó pelvic spaces
- 28. Left Supramesocolic Spaces ŌĆó The left and right supramesocolic spaces usually communicate freely with one another and include the perihepatic, left subphrenic, and perisplenic spaces ŌĆó The phrenicocolic ligament is a relative but incomplete impediment to the spread of pathologic processes from the left paracolic gutter to the left subphrenic space
- 30. Right Supramesocolic Spaces ŌĆó The right supramesocolic spaces include the: ŌĆó right subphrenic (subdiaphragmatic) space, ŌĆó the Morison pouch (subhepatic or hepatorenal space), ŌĆó the lesser sac (omental bursa).
- 31. ŌĆó The right subphrenic space is separated from the left perihepatic space by the falciform ligament, which varies in size and may not always serve as a barrier to the spread of disease ŌĆó The right subhepatic space is an important site of fluid collections resulting from liver injuries because it is the most gravity-dependent space at this site.
- 33. lesser sac ŌĆó contains a superior recess (located above the peritoneal reflection of the left gastric artery) that is in close proximity to the caudate lobe and has a boomerang-shaped recess and a larger inferior recess that lies between the stomach and the pancreatic body. ŌĆó The superior and inferior recesses are separated by a peritoneal fold that accompanies the left gastric artery.
- 35. The inferior recess communicates with a potential space between the leaves of the greater omentum. On the right side, the inferior recess communicates with the subhepatic space through the foramen of Winslow. Thus, it is possible for bowel to herniate into the lesser sac through the foramen of Winslow
- 37. Right and Left Inframesocolic Spaces ŌĆó The right and left inframesocolic spaces are separated from the supramesocolic spaces by the transverse mesocolon and from the paracolic gutters laterally by the ascending or descending colon. ŌĆó The smaller right inframesocolic space is limited inferiorly by the attachment of the small bowel mesentery to the cecum; collections in this space generally do not extend into the pelvis. ŌĆó However, the larger left inframesocolic space communicates freely with the pelvis
- 39. Paracolic Spaces ŌĆó The paracolic spaces (gutters) are located lateral to the peritoneal reflections of the left and right sides of the colon . ŌĆó The right paracolic gutter is larger than the left and communicates freely with the right subphrenic space. ŌĆó The connection between the left paracolic gutter and the left subphrenic space is partially limited by the phrenicocolic ligament. Both the right and left paracolic gutters communicate with the pelvic spaces.
- 41. Pelvic Spaces ŌĆó In men, the most gravity-dependent site for fluid accumulation is the rectovesical space. In women, it is the retrouterine space (the pouch of Douglas) . ŌĆó Anteriorly, the medial umbilical folds, which contain the obliterated umbilical arteries, divide the pelvic spaces into lateral and medial compartments. ŌĆó On each side, the inferior epigastric artery divides the lateral pelvic compartments into lateral and medial inguinal fossae, the sites of direct and indirect inguinal hernias, respectively.