














































imaging in uc and chrons disease (1).pptx
- 1. IMAGING IN ULCERATIVE COLITIS AND CHRONS DISEASE PRESENTER ŌĆō DR. VENKATESH MODERATOR ŌĆō DR. ANIL KUMAR
- 2. Introduction: ŌĆó Inflammatory bowel disease (IBD) is a fairly common enteropathy that occurs in one per 1000 people in developed countries. ŌĆó The peak incidence of IBD is between the ages of 15 and 40 years, with a possible second peak between 50 and 80 years. ŌĆó IBD is a heterogeneous group of chronic gastrointestinal disorders with two broad subtypes: Crohn disease (CD) and ulcerative colitis (UC).
- 3. ŌĆó Ulcerative colitis is characterized by relapsing and remitting episodes of inflammation limited to the colonŌĆÖs mucosal layer. It almost invariably involves the rectum, typically extends in a proximal, and continues to involve other portions of the colon. ŌĆó ChronŌĆÖs disease can involve any component of the gastrointestinal tract from the oral cavity to the anus and is characterized by trans- mural inflammation. Extensive involvement of the right colon and small intestine(Terminal ileum) is more common in CD.
- 4. Etiopathogenesis ŌĆó Highly complex and dependent on multiple factors. ŌĆó Occur in individuals who have aberrant genes which makes them abnormally susceptible to commensal bacteria which are normally present in the colon (intestinal microbiota) thus causing inflammation in the colonic mucosa. These interactions between the mucosa of the colon and colon commensals are triggered by exposure to risk factors in the environment.
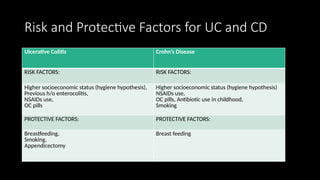
- 6. Risk and Protective Factors for UC and CD Ulcerative Colitis CrohnŌĆÖs Disease RISK FACTORS: RISK FACTORS: Higher socioeconomic status (hygiene hypothesis), Previous h/o enterocolitis, NSAIDs use, OC pills Higher socioeconomic status (hygiene hypothesis) NSAIDs use, OC pills, Antibiotic use in childhood, Smoking PROTECTIVE FACTORS: PROTECTIVE FACTORS: Breastfeeding, Smoking, Appendicectomy Breast feeding
- 7. Clinical presentation ŌĆó Diarrhea and rectal bleeding > 6 weeks (UC > CD). ŌĆó Tenesmus (Rectal inflammation). ŌĆó The severity of patient presenting with colitis can be graded as mild, moderate and severe based on the clinical presentation and physical signs.
- 8. ŌĆó Inflammatory markers : serum ŌĆō ESR stool - Fecal cal protein.
- 9. Diagnostic algorithm for confirmation of IBD diagnosis
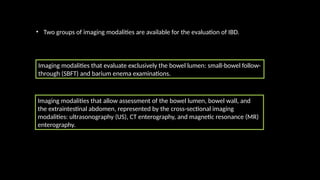
- 11. ŌĆó Two groups of imaging modalities are available for the evaluation of IBD. Imaging modalities that allow assessment of the bowel lumen, bowel wall, and the extraintestinal abdomen, represented by the cross-sectional imaging modalities: ultrasonography (US), CT enterography, and magnetic resonance (MR) enterography. Imaging modalities that evaluate exclusively the bowel lumen: small-bowel follow- through (SBFT) and barium enema examinations.
- 12. SBFT and Barium Enema Examinations ADVANTAGES ŌĆó Dynamic evaluation of the whole gastrointestinal tract ŌĆó Allows manual mobilization of the bowel DISADVANTAGES ŌĆó Ionizing radiation ŌĆó Limited in the evaluation of the intestinal wall ŌĆó It does not allow panoramic view of the abdominal cavity. ADVANTAGES ŌĆó Low cost ŌĆó Can be repeated as many times as necessary ŌĆó Absence of ionizing radiation or contrast medium DISADVANTAGES ŌĆó Operator dependent ŌĆó Limited because of intestinal gas distribution ŌĆó It does not allow panoramic view of the abdominal cavity. US Examination
- 13. CT ENTEROGRAPHY MR ENTEROGRAPHY ADVANTAGES - Thin section - Widely available - The optimal method for depicting extraluminal bowel gas and complex abdominal fistulas DISADVANTAGES - Ionizing radiation - Lower contrast resolution of the bowel wall - Intravenous iodinated contrast material necessary ADVANTAGES - High contrast resolution - Allows functional evaluations - Can be performed without the use of intravenous contrast material - The optimal method to evaluate perianal fistulas DISADVANTAGES - Higher cost and less availability - Contraindications related to the magnetic field and paramagnetic contrast material
- 14. Systemic approach ŌĆó I - Inflammatory mesentery ŌĆó B - Bowel wall changes ŌĆó D - Disease complications
- 15. B I D 1. LYMPHADENOPATHY 2. FAT CHANGES 3. ENGORGED VESSELS LUMINAL 1. STRICTURES 2. DILATATIONS 3. CANCER EXTRALUMINAL 4. FISTULA 5. ABSCESS 6. PERFORATION 1. THICKENING 2. STRATIFICATION 3. PERMANENT STRUCTURAL CHANGES
- 18. FAT STRANDING: ŌĆó The sharp interface between bowel and mesentery is lost due to influx of inflammatory cells and fluid. ŌĆó The enhancement of perienteric fat is used as a severity marker of IBD in imaging-based indices (MR imaging and Sailer index), and recent studies have shown that diffusion-weighted imaging is equivalent for the detection of small-bowel inflammation. ŌĆó Fat stranding: active inflammation marker .
- 19. FAT STRANDING:
- 20. FIBROFATTY PROLIFERATION ŌĆó Fibrofatty proliferation, also called creeping fat or fat wrapping, represents the asymmetric proliferation of fat usually along the mesenteric border, which is almost exclusively seen in CD. ŌĆó This mesenteric adipose tissue hypertrophy causes an asymmetric displacement of mesenteric vessels and isolation of the bowel from the surrounding bowel loops. ŌĆó Fibrofatty proliferation: inactive and chronic inflammation marker.
- 22. ENGORGED VASA RECTA ŌĆó Engorged vasa recta represents vascular dilatation on the mesenteric side of the bowel. ŌĆó This is also known as the ŌĆ£combŌĆØ sign because the engorged vessels have a linear appearance, resembling the teeth of a hair comb. ŌĆó Engorged vasa recta: active inflammation marker
- 24. LYMPHADENOPATHY: ŌĆó Reactive mesenteric lymphadenopathy is characterized by hyperenhancing lymph nodes that typically range from 3 to 8 mm. ŌĆó Lymphadenopatathy is commonly found in patients with IBD, both CD and UC, although it is more commonly seen with CD. ŌĆó The lymph nodes may be detected more frequently at the mesenteric root, the mesenteric periphery, or in the right lower abdominal quadrant. ŌĆó When lymph nodes are multiple and larger than 10 mm, the possibility of tumor should be considered, mainly lymphoma and carcinoma. ŌĆó Mesenteric lymphadenopathy: active inflammation marker
- 27. HOMOGENEOUS THICKENING: ŌĆó Bowel wall thickening is defined as a small bowel wall thickness greater than 3 mm in a distended loop. ŌĆó In homogeneous bowel thickening, the parietal bowel wall is enlarged without mural stratification. ŌĆó It can be asymmetric with increased thickening on the mesenteric side of the bowel, mainly in CD. ŌĆó Homogeneous thickening without enhancement may represent active or inactive inflammation marker. ŌĆó Homogeneous thickening with enhancement: active inflammation marker
- 28. BILAMINAR STRATIFICATION: ŌĆó Bowel wall thickening with bilaminar stratification results from the association of mucosal hyperenhancement and submucosal edema. ŌĆó Submucosal edema is a severity marker used in imaging-based IBD indexes. It is not specific for IBD and may be seen in other small bowel inflammatory conditions, such as ischemia and radiation enteritis. ŌĆó Bilaminar stratification: active inflammation marker
- 31. FAT HALO SIGN: ŌĆó The ŌĆ£fat haloŌĆØ sign represents infiltration of the submucosa with fat between the muscularis propria and the mucosa. ŌĆó It may be indicative of IBD, although it has been reported in cytoreductive therapy and graft-versus-host disease. ŌĆó In the absence of clinical or radiologic evidence of IBD, the presence of the fat halo sign may represent a normal finding. ŌĆó Inactive inflammation marker.
- 34. GROU P 3 DISEASE COMPLICATIONS
- 35. COLORECTAL CANCER ŌĆó Colorectal cancer has a higher incidence in patients with long-standing IBD. ŌĆó The risk is related to the duration and anatomic extent of the disease.
- 36. PITFALL: inflammatory or malignant? When we need to think of malignant wall thickening ŌĆó When thickening of bowel wall can be described as ŌĆó Focal (<5 cm) ŌĆó Irregular or asymmetric ŌĆó Heterogeneous ŌĆó Perienteric fat stranding disproportionally less severe than the degree of wall thickening When thickening of bowel wall can be described as ŌĆó Segmental or diffuse (6ŌĆō40 cm or >40 cm) ŌĆó Regular, circumferential, symmetric ŌĆó Homogeneous ŌĆó Perienteric fat stranding disproportionally more severe than the degree of wall thickening NEOPLASTIC CONDITION INFLAMMATORY CONDITION
- 39. TOXIC MEGACOLON ŌĆó Toxic megacolon is a potentially lethal complication of IBD that is characterized by total or segmental nonobstructive colonic dilatation associated with systemic toxicity. It can occur in colitis caused by UC and CD. ŌĆó The diagnosis is made by a combination of symptoms and clinical signs: ŌĆó Radiographic evidence of colonic dilatation ŌĆó Any three of the following: fever (>101.5 ┬░F), tachycardia (>120 beats per minute), leukocytosis (>10.5 x 103 /┬ĄL), or anemia ŌĆó Any one of the following: dehydration, altered mental status, electrolyte abnormality, or hypotension ŌĆó Imaging findings include: bowel wall thickening, loss of haustra, and segmental or total colonic dilatation of at least 5 cm (CT) and 8 cm (supine radiograph
- 41. PERFORATION
- 42. FISTULA ŌĆó Fistula is a permanent abnormal passageway between two organs. The clinical course is variable and depends on the location and complexity. ŌĆó Fistulas may be external (arise from the intestine and communicate with the skin) or internal (enteroenteric or between the bowel and adjacent organs). The most common fistulas are enterocutaneous and perianal. ŌĆó When compared with surgical findings, CT enterography has a reported accuracy of 86% for fistulas, with a false-negative rate of 8%.
- 43. ABSCESS
- 45. ’ā╝ Dilatation of the vasa recta ’ā╝ Fibrofatty proliferation ’ā╝Mural stratification ’ā╝ Colonic wall thickening ’ā╝ Mural thickening: 11ŌĆō13 mm, eccentric and discontinuous ’ā╝ Skip lesions (pathognomonic) ’ā╝ Right colon and terminal ileum CHRONS DISEASE ULCERATIVE COLITIS INFLAMMATORY MESENTERY BOWEL WALL CHANGES ŌĆó Dilatation of the vasa recta DISEASE COMPLICATIONS ’ā╝ Postinflammatory polyps ’ā╝ Fistulas, abscesses ’ā╝ Mural stratification ’ā╝ Colonic wall thickening ’ā╝ Mural thickening: 8 mm, symmetric and continuous ’ā╝ Postinflammatory polyps ’ā╝ Toxic megacolon
- 46. DIFFERENTIAL DIAGNOSIS: TUBERCULOSIS ISCHEMIC COLITIS
- 48. ANGIOEDEMA OF THE SMALL BOWEL PSEUDOMEMBRANOUS COLITIS
- 50. THANK YOU