


















Intestinal obstruction
- 2. ï When there is pathological interference with the normal progression of intestinal luminal contents distally the condition is called as âIntestinal obstructionâ ï Such obstruction may be due to mechanical causes (Mechanical obstruction) or âParalytic ileusâ Definition
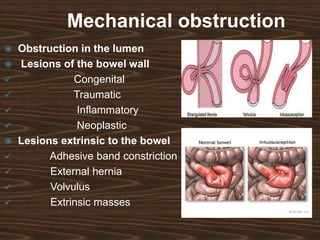
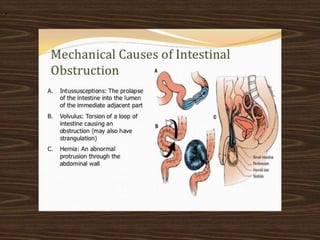
- 4. Mechanical obstruction ï Obstruction in the lumen ï Lesions of the bowel wall ïž Congenital ïž Traumatic ïž Inflammatory ïž Neoplastic ï Lesions extrinsic to the bowel ïž Adhesive band constriction ïž External hernia ïž Volvulus ïž Extrinsic masses
- 5. .
- 6. Paralytic ileus Abdominal causes Systemic causes ï Intestinal distension Electrolyte imbalance ï Peritonitis ï Retroperitoneal lesions * Retroperitoneal haemorrhage * Retroperitoneal sarcoma * Distension of ureter (Hypokalaemia)
- 7. Classification ï Simple mechanical obstruction Acute obstruction ï Strangulated obstruction Chronic obstruction ï Closed loop obstruction Acute-on-chronic obstruction
- 8. Pathology ï Bowel motility ï Distension ï Fluid and electrolyte imbalance ï Intestinal gas ï Strangulation ï Onset of gangrene ï Transmigration of bacteria and toxins
- 9. Bowel motility ï When the intestine obstructed part above the intestine shows vigorous peristalsis to overcome the obstruction. ï It remains about 2-6 days ï More distal is the obstruction more the peristalsis is and longer does it remains. ï For few hours intestines distal to the obstruction shows normal peristalsis and absorption later on it becomes immobile ï If the obstruction not relieved peristalsis ceases and intestines becomes flaccid and paralysed
- 10. Distension ï Accumulation of fluid and gas proximal to the intestinal obstruction causes intestinal distension ï Ingested fluid ï Digestive secretions ï Intestinal gas ï Plays major role in the distension
- 11. Fluid and electrolyte imbalance ï Large amount of fluid enters in to the gut daily (nearly 8000 ml/day) ï Saliva : 1500 ml ï Gastric juice : 2500 ml ï Bile & Pancreatic juice : 1000 ml and ï Intestinal juice : 3000 ml ï In intestinal obstruction distension causes increased intestinal secretion and decreased absorption ï Accumulation of such huge amount of fluid along with repeated vomiting causes severe electrolyte imbalance
- 12. Intestinal gas ï Much of the distension caused by the accumulation of gas in the intestine proximal to the obstruction. It contributes :- ï 1) Gas swallowed by atmospheric air ï 2) Diffusion of gas from blood in to lumen of the bowel (Carbon dioxide) ï 3) Organic gases : Hydrogen sulphide ï Ammonia ï Amines ï Hydrogen ï As O2 and CO2 are absorbed and Nitrogen is not absorbed, Nitrogen is highest content among the intestinal gases
- 13. Composition of various gases ï Nitrogen : 70% ï Oxygen : 12% ï Carbon dioxide : 8% ï Remaining : 10 % ï Hydrogen sulphide Ammonia and amines Hydrogen ï 5% 4% 1%
- 14. Strangulation ï When the blood circulation of affected intestine occluded strangulation develops. ï This frequently occurs in ï Adhesive band obstruction ï Hernia ï Volvulus ï Intussusception ï When the venous return is completely occluded it develops gangrene. Intestines becomes purple and then black. ï And transmition of bacteria and toxins occurres in peritoneum
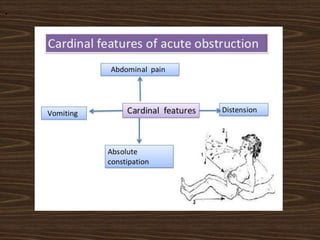
- 15. Clinical features ï Abdominal pain 1 Vomiting 2 Constipation 3 Distension 4
- 16. Abdominal pain ï This is first symptom and usually starts suddenly ï Cramping type of abdominal pain with hyper-peristalsis ï Central abdominal pain : Small intestinal obstruction ï 4-5 minutes interval in : Proximal obstruction ï 15-20 minutes interval in : Distal obstruction ï Patient is free from pain in between the attacks
- 17. Sr.No. Origin / Nature of the pain Site of obstruction 1. Diffuse, poorly localized and felt across the upper abdomen High obstruction 2. At the level of umbilicus Low ileal obstruction 3. Lower abdomen Colon obstruction 4. Perineum Recto-sigmoid obstruction 5. Continuous severe pain without any quiescent period s/o Strangulation
- 18. Vomiting ï High intestinal obstruction : Vomiting is more frequent and copious and relieved by decompression ï Lower intestinal obstruction : Vomiting is not so frequent and doesnât get relief by decompression and faeculent afterwards ï In the colon obstruction there is no vomiting until the occurrence of incompetency of valve. ï Vomiting is absent in colon obstruction until the ilio-caecal valve is competent
- 19. Constipation ï Bowel present early distal to the obstruction is evacuated and then constipation develops. ï Constipation is early in distal bowel obstruction while it is late in proximal bowel obstruction ï In few conditions of intestinal obstruction constipation is not presenting symptom for e.g.: Richterâs hernia, Intestinal obstruction in pelvic abscess, Mesenteric vascular occlusion
- 20. Distension ï Is absent in early stages ï Is much less in high small bowel obstruction ï Is centrally placed but late in low small bowel obstruction
- 21. .
- 22. .
- 23. Physical examination ï Inspection :- ï Visible peristalsis in early cases ï Abdominal distension later on Fluid thrill Shifting dullness and fullness in flanks ï All the hernial orifices must be inspected to rule out Hernia as cause of obstruction
- 24. Palpation ï Abdomen should thoroughly palpated to exclude presence of any mass which may be found in case of neoplasm, Abscess, intussusception ï Muscle guarding may be present during colic ï Tenderness and rigidity at the site of obstruction suggestive of strangulation ï Rebound tenderness suggests peritonitis and like hood strangulation ï All the hernial sites are well palpated
- 25. Auscultation ï Is having great value Sr.No. Auscultation of bowel sounds Diagnosis 1. Loud, High pitched and metallic Simple mechanical obstruction 2. Isolated bowel sound occasionally Paralytic ileus 3. Complete absence of B.S. Strangulation
- 26. Importance of rectal examination ï It should be done in all cases of intestinal obstruction. ï Presence of mass within or outside the lumen gives clue to diagnose ï Absence of faeces in the rectum suggestive of higher intestinal obstruction and vice versa ï Most of the rectal cancer are within the reach of examining finger.
- 27. Special investigations ï Blood examination ï Straight X-ray ï Barium enema ï Intravenous urography ï WBC count is very useful to differentiate type of strangulation ï Normal / Slight rise in WBC : Simple mechanical obstruction ï Moderate rise (15,000-20,000) :- Strangulation ï Very high rise (30,000-40,000) :- Primary mesenteric vascular occlusion ï Serum amylase level is often elevated (due to entry of Amylase in to blood by regurgitation from pancreas due to back pressure of duodenum)
- 28. .
- 29. Management Principle Fluid and electrolyte therapy Decompression of bowel Timed surgical intervention
- 30. .
- 31. .