













































More Related Content
What's hot (20)
Similar to Intrauterine fetal demise (20)


















Recently uploaded (20)




















Intrauterine fetal demise
- 1. INTRAUTERINE FETAL DEMISE/ DEATH KIPKORIR K NICKSON- MEDVI
- 2. ŌĆó Introduction ŌĆó Case study ŌĆó Definition of fetal death ŌĆó Epidemiology ŌĆó Aetiology ŌĆó Diagnosis/ clinical presentation ŌĆó Management ŌĆó Investigations and assessment ŌĆó Maternal studies ŌĆó Management of future pregnancy ŌĆó Summary
- 3. Introduction ŌĆó Loss of a fetus at any gestation is a fetal demise
- 4. CASE STUDY ŌĆó 29 yr para 1+0 G2 at GBD 37/40 with 1 previous scar ( emergency CS) due to fetal distress in 2014 HPI ŌĆó h/o loss of fetal movements 4/7 ŌĆó No h/o trauma, no h/o pv bleeding ŌĆó Booked at 16/40. Normal ANC follow up. Obs scan normal ŌĆó ITT injection ŌĆó On Fe supplements
- 5. PMSHX ŌĆó Non contributory FSHX Housewife. No substance us No FHx of chronic illnesses O/E Fair, afebrile, not pale/jaundiced/dehydrated/ cyanosed Vital signs; normal range P/A Pfannestiel scar, fundal height 34/40, longitudinal, cephalic, fetal heart tone absent V/E cervix 3cm long, <30% effaced, posterior, closed, firm Other systems normal
- 6. IMPRESSION; Intrauterine Fetal death at GBD 37/40 PLAN 1. Transabdominal ultasound spalding sign no fetal cardiac activity demonstrable at gestation 34 weeks 2 days 2. Arrange for delivery make decision on appropriate mode PGE2 pessary oxytocin drip (close monitoring)
- 7. Definition ŌĆó The National Centre for Health Statistics defines fetal death as death prior to the complete expulsion or extraction from its mother of a product of human conception, irrespective of the duration of pregnancy and which is not an induced termination of pregnancy ŌĆó Death is indicated by -the fetus does not breathe or show any other evidence of life - Heartbeats are to be distinguished from transient cardiac contractions
- 8. ŌĆó It is further classified as ŌĆó Early( <20 weeks gestation) ŌĆó Intermediate ( 20- 27 wks gestation) ŌĆó Late (> 28 weeks gestation)
- 9. Epidemiology ŌĆó Worldwide, rate varies considerably ŌĆó Ranging from 5 in 1000 births in high income countries and 36 in 1000 births in developing countries
- 10. Aetiology ŌĆó Any pregnancy classified as a high risk pregnancy is at risk of IUFD ŌĆó Efforts should be directed towards the recognition of such early enough ŌĆó 25-60% of fetal demise has unexplained cause ŌĆó Incidence increases with increasing gestational age
- 11. Risk factors ŌĆó African American race ŌĆó Advanced maternal age ŌĆó History of fetal demise ŌĆó Maternal colonization with certain pathogens i.e GBS, ureaplasma urealyticum ŌĆó Obesity ŌĆó Paternal age ŌĆó Male fetal sex ŌĆó Multiple gestation ŌĆó Non vertex presentation
- 12. Maternal ŌĆó Post term pregnancy (>42wks) ŌĆó Diabetes( poorly controlled) ŌĆó Systemic lupus erythematosus ŌĆó Infection, viral; Parvovirus B19, CMV, Coxsackie. Bacterial; GBS, Listeria monocytogenes, E. coli. Parasitic; Toxoplasma gondii ŌĆó Chronic hypertension ŌĆó Preeclampsia ŌĆó Haemoglobinopathy ŌĆó Advanced maternal age ŌĆó Rh disease ŌĆó Uterine rapture ŌĆó Antiphospholipid syndrome ŌĆó Maternal death
- 13. Fetal ŌĆó Multiple gestation ŌĆó Intrauterine growth restriction ŌĆó Congenital abnormality ŌĆó Infection
- 14. Placental ŌĆó Cord accident ŌĆó Abruption ŌĆó Premature rapture of membranes ŌĆó Vasa previa
- 15. Diagnosis/ Clinical presentation ŌĆó H/o decreased fetal movement ŌĆó Inability to obtain fetal heart tones upon examination suggest fetal demise ŌĆó Confirmatory: By ultrasonographic examination. - Visualize fetal heart and note absence of cardiac activity -Overlapping of skull bones (Spalding sign) - Gas in great vessels ( RobertŌĆÖs sign) - Exaggeration of fetal spinal curvature and angulation
- 16. Management Psychological ŌĆó On confirmation of diagnosis, inform patient ŌĆó Counselling- stabilize patient emotionally ŌĆó If in U/S room, allowing mother to see lack of fetal cardiac activity helps to solidify the diagnosis Definitive ŌĆó Induce labour as soon as possible ŌĆó DonŌĆÖt delay > 3-4 weeks because hypofibrinogemia develops coz thrombopastic substances are released from degenerating POCs ŌĆō risk of coagulopathy
- 17. Induction ŌĆó Cervical assesment ŌĆó Pre- induction cervical ripening followed by IV oxytocin ŌĆó In h/o previous C/S, caution coz of risk of uterine rapture ŌĆó Early fetal demise managed by MVA or Dilatation and evacuation ŌĆó < 28/40 PGE2, PGE1 +/- oxytocin ŌĆó >28/40 lower doses should be used ŌĆó Pain management- higher doses of narcotics, if superior control is needed, epidural anaesthesia should be offered
- 18. Maternal and family History ŌĆó Past obstetric history: past fetal losses ŌĆó Review history of present pregnancy -Gestational age and fetal growth - Maternal perception of fetal mvmnts in recent past -h/o bleeding - elevated blood pressure - recent illness or possible viral exposure - medications during pregnancy - substance use
- 19. Review of ANC ŌĆó Lab investigations ŌĆó Fetal assessment( NST, BPP, Doppler studies) ŌĆó Review family history
- 20. Maternal studies ŌĆó U/S ŌĆó Blood; RBS/FBS, CBC, Coagulation profile, Blood group and Ab screen, VDRL ŌĆó Urine; Toxicology ŌĆó Kleihauer- Betke ( fetal- maternal haemorrhage) 10- 15% unexplained IUFD ŌĆó TORCH screen ŌĆó Autoimmune: ANA, anticardiolipin Ab, lupus anticoagulant ŌĆó Chronic medical conditions like high TSH
- 21. Stillbirth examination a) General; -state of preservation(fresh or macerated) -wt, size and if corr to gestational age - measurements: HC, circumference of chest and abdomen, crown-heel length - Color a) Craniofacial b) Neck
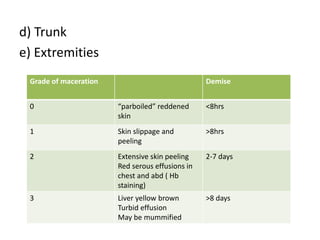
- 22. d) Trunk e) Extremities Grade of maceration Demise 0 ŌĆ£parboiledŌĆØ reddened skin <8hrs 1 Skin slippage and peeling >8hrs 2 Extensive skin peeling Red serous effusions in chest and abd ( Hb staining) 2-7 days 3 Liver yellow brown Turbid effusion May be mummified >8 days
- 23. B) Autopsy -encouraged on all stillbirths -if patients resistant to idea, limited autopsy done - Post mortem MRI can also be done C) CORD Exam -Appearance and length in cms - no. of vessels - true knots( loose or tight) - cord blood( only if fresh stillbirth) for culture and cytogenic studies( DO NOT FREEZE)
- 24. ŌĆó D) PLACENTA Exam -Gross and microscopic exam -Clinically relevant findings expected in about 30% of studied placentas -send for culture. Sterile swab btwn amnion and chorion - cytogenetic studies
- 25. ŌĆó E) Clinical PHOTOGRAPHS - Get permission from parents - Essential in documentation of both normality and abnormality tog with descriptive P/E - get AP & PA views ( whole body incl limbs - Lateral and frontal views of the face - Photos of any abnormalities
- 26. ŌĆó F) RADIOGRAPHIC Studies - useful in documenting abnormalities primarily skeletal not detected on P/E - Incl. AP plain radiograph of the whole body incl limbs( place in anatomic position) - lateral view of the skull - take separate films if structural abn are present - if dwarfism present, additional AP and lateral views of the infant limbs, head and spine
- 27. Management of future pregnancy - Preconceptional counseling is helpful if congenital anomalies or genetic abnormalities are found - Genetic screening and detailed ultrasound can evaluate future pregnancies - In cases whwere cause is unkwown, patients are naturally distressed and anxious of its recurrence - Reassurance necessary eg by increasing fetal surveillance - Optimal management of chronic medical conditions is very important prior to the next pregnancy
- 28. SUMMARY ŌĆó Loss of a fetus at any gestation is fetal demise ŌĆó Keep in mind important and most common aetiological factors ŌĆó Diagnosis ŌĆó Evaluation ŌĆó Mx of future pregnancy
- 29. THANK YOU