













intro of adr.pptx
- 1. PHARMACOVIGILANCE MISS. GAYATRI K. BAHATKAR ASSISTANT PROFESSOR P. R. PATIL INSTITUTE OF PHARMACY , TALEGOAN SP.
- 2. INTRODUCTION TO ADVERSE DRUG REACTIONS âĒ Adverse drug reactions (ADRs) is an unwanted, undesirable effect of a medicine that occurs during usual clinical application. It occurs almost daily in health care institutions and can adversely affect a patientâs quality of life; sometimes may lead to considerable morbidity and mortality. Much attention has been given to identify The patient populations most at risk, The drugs most commonly responsible, and The potential causes of ADRs. The factors responsible for the prevalence of ADRs worldwide are: âĒ Increase in the number of drugs in the market, âĒ An aging population, and âĒ An upward trend in polypharmacy.
- 3. âĒ The difference between ADRS and ADES is that ADRs can occur even after appropriate prescription and correct dosing. ADES are generally associated with inappropriate use of the drug that usually occurs during drug therapy. It may not be related to the pharmacology o the drug itself. Adverse drug events (ADES) may occur due to medication errors. The National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) has defined the medication errors as: âany preventable event that may cause or lead inappropriate medication use or patient harm while the medication is in the control of the Health care professional, patient, or consumer.
- 4. Objectives of ADRs Monitoring âĒ (A) To help the drug regulatory authority, public health programmes, scientists and consumers for taking appropriate action to reduce the risks of ADRs. It is also necessary to find out the nature and frequency of ADRs with periodical check of the benefit-risk ratio of medicinal products. The benefit-risk ratio of medicinal products can be re for evaluated by: âĒ Providing updated drug safety information to health care professionals and other stakeholders including WHO ADRs Monitoring Centers. âĒ Updating information in package and disseminating information which may result recall or withdrawal of the product in the market or restrictions for marketing. âĒ Propagating information for designing proper education programme to consumers and other users. âĒ Taking initiative to study the effect of a for further education. For example benefit of the drug especially in long term for prevention of relapse or study of new indication, overuse, possible mechanism underlying the adverse reaction observed or misuse.
- 5. âĒ (B) To identify the risk factors that may affect, induce or influence the development, severity and incidence of adverse reactions in the population; for example, âĒ 1 Patient factors such as genetics, racial differences, diets, diseases, prescribing Practices, pattern of drug use and food habits (high carbohydrate, fat diet etc.). âĒ 2. Drug interactions, drug distribution, storage and use including indications, dose. Availability and other underlying conditions. âĒ Due to adverse drug reactions the patients may lose confidence in the therapy or may show negative towards their physicians and may look for self-treatment options. As a result additional ADRS may not be observed. About 5% of the hospital admissions are the result of an ADR, and at least one ADR would be found in about 10%-20% of inpatients during their stay in hospitals. The actual frequency of ADRS may be even greater than the above values. Because some
- 6. âĒ Some ADRs present minor symptoms, others are serious and cause death in as many as 0.1%-0.3% of hospitalized patients. âĒ Adverse drug reactions should be identified and managed as early as possible to reduce their harmful effects on the patients. The cost of managing ADRs can be high, whether they occur in the inpatients or the outpatients. The clinical diagnosis of an ADR is not always observable. Practitioners often advise Additional laboratory tests or procedures to investigate the cause of a patientâs symptoms. âĒ Practitioners may also prescribe pharmacotherapy for conditions caused by an unrecognized ADR. This increases the cost of treatment as well as the risk of additional ADRs. âĒ If the ADR occurs when the patient is hospitalized, the duration of stay can be increased and overall cost of treatment may also increase. âĒ Due to ADRs the anxiety or depression and loss of working days for the Patient and/or Caregiver may take place, as a result additional indirect cost may increase.
- 7. âĒ The study of drug-related injuries and making warning or withdrawal recommendations for pharmaceutical agents are the major activities of pharmacovigilance; however, it includes assessment, understanding, and prevention of ADRs. âĒ Pharmacists play a vital role in each step of the pharmacovigilance activity; so that the Patients need not require unnecessary procedures or take unnecessary drugs so that safety And quality of life for the patient can be preserved.
- 8. DEFINITIONS AND CLASSIFICATION OF ADRS âĒ According to the World Health Organization (WHO) an ADR is defined as "a response to a drug which is noxious and undesired and which occurs at normal doses when used in man for prophylaxis, diagnosis, or therapy of disease or for the modification of physiologic function. Thus, an ADR is a type of ADE whose cause can be directly related to a drug and its physiologic properties. âĒ In many cases it may be observed that a particular patient develops an adverse drug reaction, while another patient does not. There is no specific reason for this. There are some relatively toxic drugs which show adverse reactions in most cases. This can be considered as the rule rather than the exception. Four special
- 9. âĒ comprising inherent anomalies in patient response (allergic or idiosyncratic), âĒ Acquired patient anomalies, âĒ Anomalies of drug presentation, and âĒ Anomalies in administration, and interactions. Etiology âĒ Most of the adverse drug reaction and dose related . Others are allergic or idiosyncratic dose- related ADRs are usually predictable âĒ Dose related ADRs are particularly of concern when drug have narrow therapeutic index. For example, haemorrhage and oral anticoagulant . ADRs may occurs due to decreased drug clearance in patient with impaired renal or hepatic function due to drug drug
- 10. âĒ Allergic ADRs are not dose-related and require prior exposure. Allergies develop when a drug acts as an antigen or allergen. After a patient is sensitized, subsequent exposure to the drug produces one of several different types of allergic reaction. Clinical history and appropriate skin tests can sometimes help to predict allergic ADRs. âĒ Idiosyncratic ADRs are unexpected ADRs that are not dose-related or allergic. They occur in small number of patients when a drug is administered. Idiosyncrasy is not a precise term. It is defined as a genetically determined abnormal response to a drug. However, all idiosyncratic reactions do not have a pharmacogenetic cause. The term may become obsolete when specific mechanisms of ADRS are known.
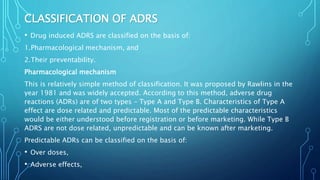
- 11. CLASSIFICATION OF ADRS âĒ Drug induced ADRS are classified on the basis of: 1.Pharmacological mechanism, and 2.Their preventability. Pharmacological mechanism This is relatively simple method of classification. It was proposed by Rawlins in the year 1981 and was widely accepted. According to this method, adverse drug reactions (ADRs) are of two types â Type A and Type B. Characteristics of Type A effect are dose related and predictable. Most of the predictable characteristics would be either understood before registration or before marketing. While Type B ADRS are not dose related, unpredictable and can be known after marketing. Predictable ADRs can be classified on the basis of: âĒ Over doses, âĒ Adverse effects,
- 12. âĒ Drug-drug interaction, and âĒ Drug-disease interaction. Unpredictable ADRs may happen due to: âĒ Intolerance, âĒ Allergy, âĒ Pseudo-allergy, and âĒ Idiosyncrasy. However, there are other methods of classification of ADRs. These including Type A and Type B classification are tabulated below. Classification according to Rawlins is shown below.
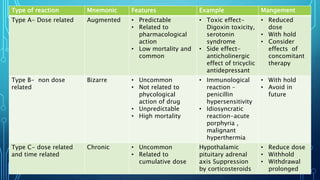
- 13. Type of reaction Mnemonic Features Example Mangement Type A- Dose related Augmented âĒ Predictable âĒ Related to pharmacological action âĒ Low mortality and common âĒ Toxic effect- Digoxin toxicity, serotonin syndrome âĒ Side effect- anticholinergic effect of tricyclic antidepressant âĒ Reduced dose âĒ With hold âĒ Consider effects of concomitant therapy Type B- non dose related Bizarre âĒ Uncommon âĒ Not related to phycological action of drug âĒ Unpredictable âĒ High mortality âĒ Immunological reaction â penicillin hypersensitivity âĒ Idiosyncratic reaction-acute porphyria , malignant hyperthermia âĒ With hold âĒ Avoid in future Type C- dose related and time related Chronic âĒ Uncommon âĒ Related to cumulative dose Hypothalamic pituitary adrenal axis Suppression by corticosteroids âĒ Reduce dose âĒ Withhold âĒ Withdrawal prolonged
- 14. Type D â time related Delayed âĒ Uncommon âĒ Usually dose related âĒ Occurs or become apparent sometime after use of drug Teratogenesis carcinogenesis Tardive dyskinesia Often difficult to manage Type E- withdrawal End of use âĒ Uncommon âĒ Occurs some after âĒ Withdrawal of drug âĒ Opiate withdrawal syndrome âĒ Myocardial ischemia Reintroduced or Withdraw slowly Type F- unexacted failure of therapy Failure âĒ Common âĒ Dose related âĒ Often caused by drug interaction âĒ Oral contraceptive when used with enzyme inducer âĒ Increased dose âĒ Consider effect of concomitant therapy
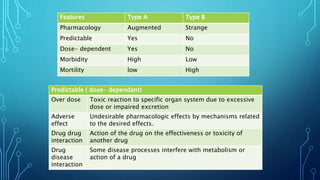
- 15. Features Type A Type B Pharmacology Augmented Strange Predictable Yes No Dose- dependent Yes No Morbidity High Low Mortility low High Predictable ( dose- dependant) Over dose Toxic reaction to specific organ system due to excessive dose or impaired excretion Adverse effect Undesirable pharmacologic effects by mechanisms related to the desired effects. Drug drug interaction Action of the drug on the effectiveness or toxicity of another drug Drug disease interaction Some disease processes interfere with metabolism or action of a drug
- 16. Unpredictable ( dose independent ) Intolerance Overstated, sometimes disabling effects even when the drug is given in Usual doses Idiosyncrasy Abnormal reactions to a drug related to metabolic or enzyme deficiency Which can be genetically determined, or altered activation/detoxification Pathways. Allergy Reaction is Specific to a given Drug, Severe, Recurrent And Immunologically mediated Pseudo-allergy Clinically it is similar to allergic reactions, but involves an unknown immune mechanism
- 17. PHARMACOLOGICAL CLASSIFICATION ACCORDING TO GRUCHALLA Type of ADRs Example Type A reactions: predictable Toxicity or overdose Hepatic failure with high-dose paracetamol. Side effects Sedations with antihistamines. Secondary effect Diarrhea with antibiotic such as Ampicillin due to alteration of Gastrointestinal bacterial flora. Drug interaction Toxicity of theophylline in presence of erythromycin therapy. Type B reaction : unpredictable Intolerance Tinnitus with use of aspirin. Idiosyncratic reaction Occurrence of anemia with use of an antioxidant drug in Presence of glucose-6-phosphate dehydrogenase deficiency. Immunological Hypersensitivity reaction Anaphylaxis with penicillin administration. Pseudo-allergic reaction (non immunological) Radio contrast dye reaction.
- 18. PHARMACOLOGICAL CLASSIFICATION ACCORDING TO GHARAIBEH: Feature Type 1 Type 2 Synonyms Augmented, predictable, Toxic, quantitative, dose Related. Strange, unpredictable, idiosyncratic, allergic, drug- intolerance, qualitative, Dose- independent. Mechanism Understood, predictable Generally poorly understood Site (a)Same site of primary drug action (b)another site for primary and secondary actions Usually the site of action is not Related Incidence High (70%) Low (30%) Morbidity Severe Mortality Mortality Low High Causes Pharmaceutica l dosage form Increased availability at the site of absorption: quantity and release of dosage form Decomposition products, additives excipients, etc. Pharmacokine tic Amount of drug Increased at the site of action due to Abnormalities in ADME Liberation of an abnormal metabolite
- 19. Pharmacodynamic (a)Response of organ or tissue increased due to number sensitivity of receptors (b) Homeostatic imbalance (C)Diseases state (a) Genetic (b) Immunologic (c) Neoplastic (d) Teratologic Reproducibility Reproducible Not reproducible Treatment Dose to be adjusted Treatment to be discontinued
- 20. PHARMACOLOGICAL CLASSIFICATION ACCORDING TO ROYER & STEPHENS Type Characteristics Type A Reactions that result from exaggerated pharmacological action of a drug given as normal therapeutic doses usually dose dependent. Sometimes referred to as Type 1. Type B Represents a new or novel response different from usual pharmacologic action â sometimes referred to as Type 2. Type C Adaptive changes, rebound phenomena, other long-term effects Type D Carcinogenesis, effects concerned with reproduction (impaired fertility). Teratogenesis (adverse effects on the fetus during early stages of pregnancy), adverse effects on the fetus during later stages of pregnancy, drug in breast milk.
- 21. PHARMACOLOGICAL CLASSIFICATION ACCORDING TO WILLS & BROWN: Type Characteristics A Dose related, pharmacologically predictable, commonly improves after Withdrawal of medicine. B Involves interaction with a microorganism, pharmacologically predictable, commonly improves after withdrawal of medicine. C An Irritant reaction, related to concentration of a drug D Depends on the route of administration or nature of formulation, improves if the medicine is withdrawn or route of administration is Changed. E Begins when medicine is Stopped Or The Dose Reduced, Pharmacologically predictable F Occurs only in those genetically predisposed, improves if the medicine is Withdrawn. G Causes irreversible genetic damage. H Requires activation of immune system, improves if the medicine is withdrawn. U Mechanism is not understood