Joint examination
•Download as PPTX, PDF•
14 likes•8,224 views

How to perform joint examination general scheme general rules , inspection , palpation , movement ,special tests





Joint examination
- 2. Objectives • General rules • Components of joint examination • Closure of the station
- 3. C L I N I C A L D A Y General rules • Introduce your self. • Clarifying the purpose of the meeting. • Offer analgesia. • Clean your hands. • Brief focused history.
- 4. C L I N I C A L D A Y Components of joint examination • Look (inspection) • Feel (palpation) • Move: – Active movements – Passive movements – Grading muscular power • Special tests • Neurovascular assessment
- 5. C L I N I C A L D A Y Look(inspection) • General resting posture and/or gait • Skin • Subcutaneous tissue • Muscle and tendons • Bone • Joint
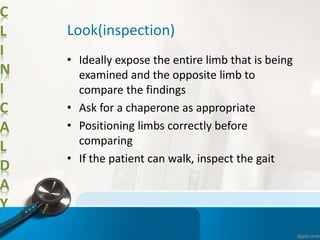
- 6. C L I N I C A L D A Y Look(inspection) • Ideally expose the entire limb that is being examined and the opposite limb to compare the findings • Ask for a chaperone as appropriate • Positioning limbs correctly before comparing • If the patient can walk, inspect the gait
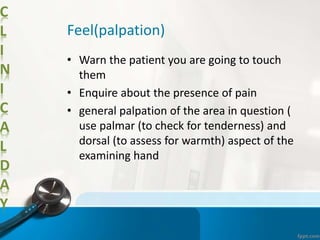
- 7. C L I N I C A L D A Y Feel(palpation) • Warn the patient you are going to touch them • Enquire about the presence of pain • general palpation of the area in question ( use palmar (to check for tenderness) and dorsal (to assess for warmth) aspect of the examining hand
- 8. C L I N I C A L D A Y Feel(palpation) • Palpate bony landmarks, muscle and tendon groups and any major nerves • Localized tenderness ---injury or inflammation of a particular structure • Diffuse tenderness ---general process like cellulitis or arthritis • Palpate for a joint effusion.
- 9. C L I N I C A L D A Y Movement • Active movements • Assisted movements • Passive movements • Power
- 10. C L I N I C A L D A Y Special test • Shoulder ---- rotator cuff, signs of impingement and instability • Knee---extensor mechanism, the collateral and cruciate ligaments, and menisci and look for signs of patella-femoral dysfunction. • Hip----fixed deformities, particularly Thomas’ test for fixed flexion
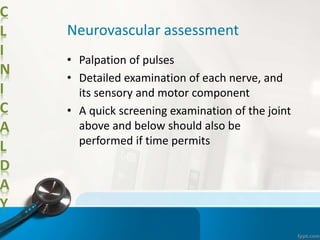
- 11. C L I N I C A L D A Y Neurovascular assessment • Palpation of pulses • Detailed examination of each nerve, and its sensory and motor component • A quick screening examination of the joint above and below should also be performed if time permits
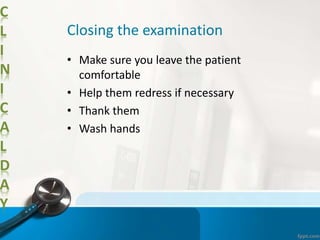
- 12. C L I N I C A L D A Y Closing the examination • Make sure you leave the patient comfortable • Help them redress if necessary • Thank them • Wash hands
- 14. C L I N I C A L D A Y Summary • General rules • Inspection • Palpation • Movement • Special tests • Neurovascular assessment • Closure
Editor's Notes
- #6: General resting posture and/or gait: general attitude of the limb (limb positioning) - this provides clues to tendon injury, disc prolapse, fracture, muscle weakness. •• Skin: scars, sinuses, swellings, contractures, erythema/colour change, atrophy, loss of hair or nail, ulceration. •• Subcutaneous tissue: oedema, contractures, haematoma, swellings. •• Muscle and tendons: atrophy, hypertrophy, contractures, bulge (Popeye sign of biceps rupture), tendon ruptures, muscle haematoma. •• Bone: deformity, swelling, shortening. •• Joint: deformity, shortening, contractures, effusion.
- #10: Active movements: the patient should be systematically directed to move the joint themselves. The range of movement can be compared to the normal side to measure the extent of any limitation. Checking active movements first also helps to localise any areas of concern which the clinician can then focus on while checking movements passively. •• Assisted movements: this is where the patient moves the limb but some assistance may be provided by the examiner to take the joint through its full range of motion. This is especially relevant in shoulder examination when demonstrating a painful arc or a ruptured rotator cuff. •• Passive movements: after checking active movements, passive movements can then be checked by the examiner moving the limb/joint in question. This is useful as sometimes the patient may not be able to move a limb due to muscle/tendon injury or paralysis. However, the presence of a full passive range of movement indicates the absence of any injury to the joint itself. With passive movement, one should also be able to feel for any crepitus by resting a hand on the joint during movement. •• Power: finally the power of muscle groups should be tested and graded as per the medical research council scale (see page 134). It should be clear as to whether power is reduced because of true neurological weakness or due to pain.