Kids Camp Registration Form
3 likes6,232 views

(1) This document provides registration information for a summer kids' camp taking place from August 22-28, 2010. It includes forms for camper medical history, permission, and medication dosing. (2) Campers must submit a $100 non-refundable deposit by July 1 for early registration, or pay the full $225 fee for late registration after July 1. Final payments are due by July 22. (3) The forms request medical information, permission to administer typical over-the-counter medications, and details on any prescription medications the camper will bring to ensure proper dosing.

![Seattle District of Foursquare Churches Summer Camp
Medication Dosing Form
If your camper will be bringing ANY prescription or non-prescription medication to camp, please complete this form to help us
ensure all students receive medication on the proper schedules. All medications must be turned in to and will be administered by
the camp nurse.
Please list all medications your camper will be bringing. Please indicate if the medication is ŌĆ£AS NEEDEDŌĆØ in the Other Times"
column.
Camper Name:
Camper Church:
Parent Name:
Parent Contact:
Cabin Number: Camp Use Only
Cabin Leader: Camp Use Only
Medication Purpose Notes/Comments Dose Amount Breakfast Lunch Dinner Bedtime Other Times
CIRCLE TIMES WHEN MEDICATION MUST BE GIVEN
BREAKFAST LUNCH DINNER BEDTIME
Camp Use Only M[ ] T[ ] W[ ] Th M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] Th[ ]
(X after meds are given) [ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] F[ ] S[ ]
BREAKFAST LUNCH DINNER BEDTIME
Camp Use Only M[ ] T[ ] W[ ]Th M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] Th[ ]
(X after meds are given) [ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] F[ ] S[ ]
BREAKFAST LUNCH DINNER BEDTIME
Camp Use Only M[ ] T[ ] W[ ] Th M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] Th[ ]
(X after meds are given) [ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] F[ ] S[ ]
BREAKFAST LUNCH DINNER BEDTIME
Camp Use Only M[ ] T[ ] W[ ] Th M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] Th[ ]
(X after meds are given) [ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] F[ ] S[ ]](https://image.slidesharecdn.com/kcregistrationform-1278459214-phpapp02/85/Kids-Camp-Registration-Form-3-320.jpg)
Kids Camp Registration Form
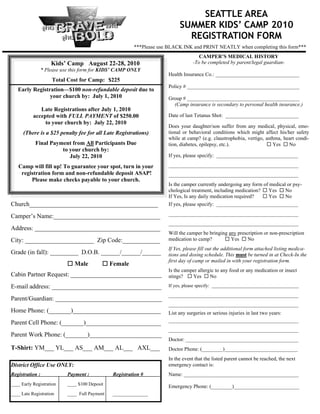
- 1. SEATTLE AREA SUMMER KIDSŌĆÖ CAMP 2010 REGISTRATION FORM ***Please use BLACK INK and PRINT NEATLY when completing this form*** CAMPERŌĆÖS MEDICAL HISTORY KidsŌĆÖ Camp August 22-28, 2010 -To be completed by parent/legal guardian- * Please use this form for KIDSŌĆÖ CAMP ONLY Health Insurance Co.: ________________________________ Total Cost for Camp: $225 Policy # ___________________________________________ Early RegistrationŌĆö$100 non-refundable deposit due to your church by: July 1, 2010 Group # ___________________________________________ (Camp insurance is secondary to personal health insurance.) Late Registrations after July 1, 2010 accepted with FULL PAYMENT of $250.00 Date of last Tetanus Shot: ____________________________ to your church by: July 22, 2010 Does your daughter/son suffer from any medical, physical, emo- (There is a $25 penalty fee for all Late Registrations) tional or behavioral conditions which might affect his/her safety while at camp? (e.g. claustrophobia, vertigo, asthma, heart condi- Final Payment from All Participants Due tion, diabetes, epilepsy, etc.). ’é© Yes ’é© No to your church by: July 22, 2010 If yes, please specify: _______________________________________ Camp will fill up! To guarantee your spot, turn in your ______________________________________________________________ registration form and non-refundable deposit ASAP! ______________________________________________________________ Please make checks payable to your church. Is the camper currently undergoing any form of medical or psy- chological treatment, including medication? ’é© Yes ’é© No If Yes, Is any daily medication required? ’é© Yes ’é© No Church_________________________________________ If yes, please specify: _______________________________________ ______________________________________________________________ CamperŌĆÖs Name:__________________________________ ______________________________________________________________ Address: ________________________________________ Will the camper be bringing any prescription or non-prescription City: ______________________ Zip Code:____________ medication to camp? ’é© Yes ’é© No If Yes, please fill out the additional form attached listing medica- Grade (in fall): _________ D.O.B. ______/______/______ tions and dosing schedule. This must be turned in at Check-In the h first day of camp or mailed in with your registration form. ’é© Male ’é© Female h Is the camper allergic to any food or any medication or insect Cabin Partner Request: _____________________________ stings? ’é© Yes ’é© No E-mail address: ___________________________________ If yes, please specify: _____________________________________ ______________________________________________________________ Parent/Guardian: __________________________________ ______________________________________________________________ Home Phone: (_______)____________________________ List any surgeries or serious injuries in last two years: ______________________________________________________________ Parent Cell Phone: (_______)________________________ ______________________________________________________________ Parent Work Phone: (_______)_______________________ Doctor: ___________________________________________ T-Shirt: YM___ YL___ AS___ AM___ AL___ AXL___ Doctor Phone: (________)____________________________ In the event that the listed parent cannot be reached, the next District Office Use ONLY: emergency contact is: Registration : Payment : Registration # Name: ____________________________________________ ____ Early Registration ____ $100 Deposit Emergency Phone: (________)_________________________ ____ Late Registration ____ Full Payment _______________
- 2. KIDSŌĆÖ CAMP SUMMER CAMP 2010 Permission Slip and Medical Release CamperŌĆÖs Name Printed: __________________________ Age: ______ CamperŌĆÖs Church: _________________________ THIS REGISTRATION IS NOT VALID WITHOUT THE FOLLOWING TWO SIGNATURES: 1. Campers Declaration: I will fully cooperate with the staff, rules and program established for the camp so as to not discredit my parents, my church or myself. CamperŌĆÖs Signature: ___________________________________________________________________ Date: ______/______/______ 2. Parental Release: I agree that my above-named son/daughter may attend the Seattle Area Foursquare Churches Summer Camp at Lake Retreat in Ravensdale, WA and agree to him/her taking part in all of the activities described below, with the exception of those listed. I acknowledge that these activities involve the risk of serious injury or death. I acknowledge the need for responsible behavior and obedience on his/her part. The program may include: water activities (such as swimming, the blob, etc... in which students would be participating in at the lake), sporting activities/all camp games/team sports/field games (such as flag football, basketball, dodge ball, volleyball, softball, mini-golf, Frisbee-golf), and mingling with other individuals and groups. Specific activities may be excluded or addedŌĆöplease contact the Camp Director if you have any questions or concerns. Please exclude my child from participating in: ________________________________________________________________ _______________________________________________________________________________________________________ I give permission for staff to give my son/daughter the following: Acetaminophen - Tylenol or Generic: ’é© Yes ’é© No Aspirin: ’é© Yes ’é© No Ibuprofen - Advil or Generic: ’é© Yes ’é© No Antihistamine - Benadryl or Generic: ’é© Yes ’é© No Cough Suppressant - Robitussin or Generic: ’é© Yes ’é© No Decongestant - Sudafed or Generic: ’é© Yes ’é© No Hydrocortisone Ointment: ’é© Yes ’é© No Antibiotic Ointment: ’é© Yes ’é© No Antacid - TUMS, Mylanta, Maalox or Generic: ’é© Yes ’é© No I understand that I am responsible for my childŌĆÖs actions and will be held financially responsible for any damage done by my child and will pay for any and all repairs incurred by such damage. I give permission for media shots of my child to be used for Summer Camp informational and promotional purposes. I give consent for my child to go on Seattle District Camp authorized field trips away from camp premises. I give permission for my child to ride in chartered buses or vehicles used for camp trips or camper transport. I understand that the deposit submitted with this application is non-refundable (contact your church about the possibility of transferring it to another student). I understand that the last day to cancel participation to receive back the refundable portion of camp cost is July 22, 2010 for Seattle District KidsŌĆÖ Camp. I will contact the Camp Administrator directly to cancel participation and understand that fees will be refunded to my church, and they will refund me. Declarations In the event of an accident or an illness during this event that needs immediate treatment, I agree to my son/daughter receiving first aid & medical treatment from qualified practitioners, including life-saving treatments, as may be considered necessary by a licensed medical provider. I also authorize the transportation of my child, by ambulance if necessary, to the nearest available medical facility. I understand the extent & limitations of the insurance coverage as provided by the organization sponsoring the event, and that my medical insurance is pri- mary, unless otherwise specified. I will inform the leaders of the event as soon as possible if there is any change in medical circumstances regarding my child between the date signed below and the start of this event. Signature: ___________________________________________________________________ Date: ______/______/______ Name Printed: _________________________________________________________________________________________ Coming Late or Leaving Early: Transportation to Lake Retreat is not provided. Unusual situations which require the camper to arrive late at camp or depart early, require an additional release to be submitted to the Camp Administrator. Please complete page four and mail it to the address on the bottom of the form.
- 3. Seattle District of Foursquare Churches Summer Camp Medication Dosing Form If your camper will be bringing ANY prescription or non-prescription medication to camp, please complete this form to help us ensure all students receive medication on the proper schedules. All medications must be turned in to and will be administered by the camp nurse. Please list all medications your camper will be bringing. Please indicate if the medication is ŌĆ£AS NEEDEDŌĆØ in the Other Times" column. Camper Name: Camper Church: Parent Name: Parent Contact: Cabin Number: Camp Use Only Cabin Leader: Camp Use Only Medication Purpose Notes/Comments Dose Amount Breakfast Lunch Dinner Bedtime Other Times CIRCLE TIMES WHEN MEDICATION MUST BE GIVEN BREAKFAST LUNCH DINNER BEDTIME Camp Use Only M[ ] T[ ] W[ ] Th M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] Th[ ] (X after meds are given) [ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] F[ ] S[ ] BREAKFAST LUNCH DINNER BEDTIME Camp Use Only M[ ] T[ ] W[ ]Th M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] Th[ ] (X after meds are given) [ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] F[ ] S[ ] BREAKFAST LUNCH DINNER BEDTIME Camp Use Only M[ ] T[ ] W[ ] Th M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] Th[ ] (X after meds are given) [ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] F[ ] S[ ] BREAKFAST LUNCH DINNER BEDTIME Camp Use Only M[ ] T[ ] W[ ] Th M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] M[ ] T[ ] W[ ] Th[ ] (X after meds are given) [ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] Th[ ] F[ ] S[ ] F[ ] S[ ]