













kista ovarium susp malignancy, diare kronik e.c maligancy,.pptx
- 1. DEATH CASE C2 WARD Admission : 31st December 2021 (09.30) Time of death: 31st December 2021 (17.45)
- 3. Patient Identity Name : Mrs. CS Age : 63 y.o Gender : Female Profession : Housewife Education : Senior High School
- 4. Present Medical History • Chief Complaint: Liquid stool
- 5. Present Medical History • Liquid stool 6-7x a day, for the last 2 weeks • The consistency is liquid + , yellowish brown +, black blood denied -, nausea - vomiting -, decreased appetite +. • There is weight loss in the last month but not measured • fever cough tightness denied by the patient, urination normal, • intermittent abdominal pain + in the last mont, history of an ovarian cyst since 1 year ago • elective surgery plan today but canceled because the patient has liquid stool. • Recuring vaginal spotting since 1 year ago and now the patient have vaginal spotting in the last 3 weeks.
- 6. Past Medical History • History of type 2 DM denied • History of Hypertension since 2 years ago, treated with amlodipine 1x5mg • History of asthma since 3 years ago, use berotec 3x1 puff if having shortness of breath. • The patient was planned for HTSOB on 29/12/21 but it was canceled because the patient was being treated in the internal department because of diarrhea
- 7. Family Medical History • None experienced the same illness
- 8. Physical Examination • General condition: Moderately ill • Sensorium: Compos Mentis • BP: 130/85 mmHg, HR 72x/m, RR 24 x/m, T 36,0°C SpO2 98% room air • BW 75 kg; BH 165 cm BMI : 27,54 kg/m2 • Eye : anemic conjunctiva -, icteric sclera -, • Neck: JVP distended (-), no lymph nodes enlargement
- 9. Physical Examination • Lung: – Inspection : symmetrical chest movement – Palpation : Stem fremitus R=L – Percussion : Sonor – Auscultation : vesicular breath sound +/+, rhonchi -/-, wheezing -/- • Heart: – Inspection : Ictus cordis not visible – Palpation : Ictus cordis not palpable – Percussion : left border: ICS V left midclavicularis line – right border: ICS IV right parasternalis line – Auscultation : regular I –II heart sound, no murmur nor gallop
- 10. Physical Examination • Abdomen: – Inspection : distended – Auscultation : normal bowel sound – Percussion : Dim, Shifting dullnes (+) – Palpation : no liver and spleen enlargement, undulation +, palpable imobile mass at the level of umbilicus, minimal tenderness – Extremities: warm, edema -/-, CRT <2”
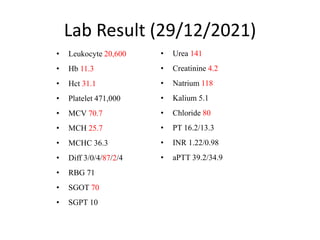
- 11. Lab Result (29/12/2021) • Leukocyte 20,600 • Hb 11.3 • Hct 31.1 • Platelet 471,000 • MCV 70.7 • MCH 25.7 • MCHC 36.3 • Diff 3/0/4/87/2/4 • RBG 71 • SGOT 70 • SGPT 10 • Urea 141 • Creatinine 4.2 • Natrium 118 • Kalium 5.1 • Chloride 80 • PT 16.2/13.3 • INR 1.22/0.98 • aPTT 39.2/34.9
- 12. CS-SCAN Abdomen
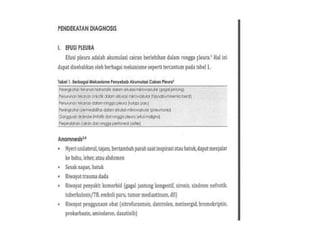
- 13. Abdominal CT-Scan (21/12/2021) • Malignant mass in the pelvic cavity, impression comes from the reproductive organs that extends to the abdominal cavity, pressing the loops of the intestine and the surrounding ureter, sticking to the mesentery and peritoneal walls accompanied by multiple lymphadenopathy parametrium, paraaorta abdominalis and mesentery • Mild hydronephrosis bilateral • Right pleural effusion
- 14. Chest X-Ray
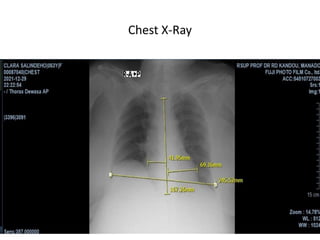
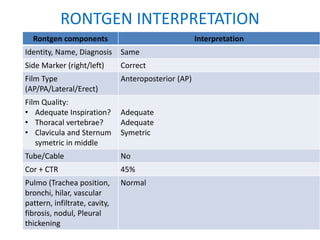
- 15. RONTGEN INTERPRETATION Rontgen components Interpretation Identity, Name, Diagnosis Same Side Marker (right/left) Correct Film Type (AP/PA/Lateral/Erect) Anteroposterior (AP) Film Quality: • Adequate Inspiration? • Thoracal vertebrae? • Clavicula and Sternum symetric in middle Adequate Adequate Symetric Tube/Cable No Cor + CTR 45% Pulmo (Trachea position, bronchi, hilar, vascular pattern, infiltrate, cavity, fibrosis, nodul, Pleural thickening Normal
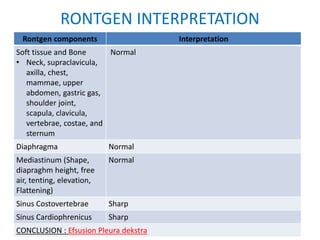
- 16. RONTGEN INTERPRETATION Rontgen components Interpretation Soft tissue and Bone • Neck, supraclavicula, axilla, chest, mammae, upper abdomen, gastric gas, shoulder joint, scapula, clavicula, vertebrae, costae, and sternum Normal Diaphragma Normal Mediastinum (Shape, diapraghm height, free air, tenting, elevation, Flattening) Normal Sinus Costovertebrae Sharp Sinus Cardiophrenicus Sharp CONCLUSION : Efsusion Pleura dekstra
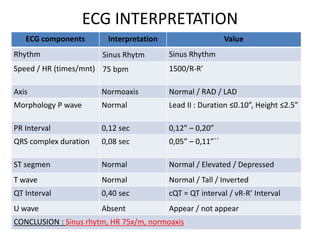
- 17. ECG
- 18. ECG INTERPRETATION ECG components Interpretation Value Rhythm Sinus Rhytm Sinus Rhythm Speed / HR (times/mnt) 75 bpm 1500/R-R’ Axis Normoaxis Normal / RAD / LAD Morphology P wave Normal Lead II : Duration ≤0.10”, Height ≤2.5” PR Interval 0,12 sec 0,12” – 0,20” QRS complex duration 0,08 sec 0,05” – 0,11”`` ST segmen Normal Normal / Elevated / Depressed T wave Normal Normal / Tall / Inverted QT Interval 0,40 sec cQT = QT interval / vR-R’ Interval U wave Absent Appear / not appear CONCLUSION : Sinus rhytm, HR 75x/m, normoaxis
- 19. Medical Diagnosis • Chronic diarrhea ec suspected malignancy • Susp malignant ovarian cyst • Right pleural effusion • Hyponatremia • AKI dd CKD 5 ND ec obstructive nephropathy dd HNS. • hypertension
- 20. Pharmacological Instruction • Nacl 0.9% 1500cc: kidmin 200cc /24hours • Ciprofloxacin 400 mg/12 hours IV ST • Omeprazol 40 mg/12 hours IV • new diatab 3x2tablet Po • amlodipine 1x5mg Po • Bicnat 3 x 500 mg Po
- 21. Non Pharmacological Instructions • Monitoring Vital sign/8 hr • Monitor urine output/24hr • Fluid balance • Check complete stool + BT • Check urinalysis • USG abdomen and renal • Check Ca, Mg, P, Albumin • Consult obsgyn • Consult surgeon
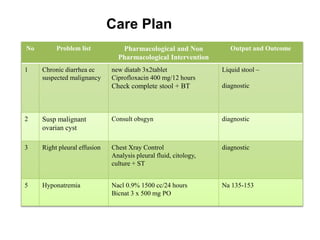
- 22. Care Plan No Problem list Pharmacological and Non Pharmacological Intervention Output and Outcome 1 Chronic diarrhea ec suspected malignancy new diatab 3x2tablet Ciprofloxacin 400 mg/12 hours Check complete stool + BT Liquid stool – diagnostic 2 Susp malignant ovarian cyst Consult obsgyn diagnostic 3 Right pleural effusion Chest Xray Control Analysis pleural fluid, citology, culture + ST diagnostic 5 Hyponatremia Nacl 0.9% 1500 cc/24 hours Bicnat 3 x 500 mg PO Na 135-153
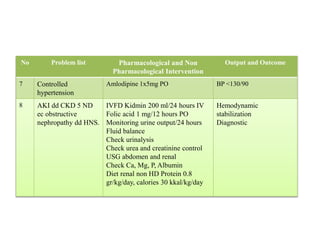
- 23. No Problem list Pharmacological and Non Pharmacological Intervention Output and Outcome 7 Controlled hypertension Amlodipine 1x5mg PO BP <130/90 8 AKI dd CKD 5 ND ec obstructive nephropathy dd HNS. IVFD Kidmin 200 ml/24 hours IV Folic acid 1 mg/12 hours PO Monitoring urine output/24 hours Fluid balance Check urinalysis Check urea and creatinine control USG abdomen and renal Check Ca, Mg, P, Albumin Diet renal non HD Protein 0.8 gr/kg/day, calories 30 kkal/kg/day Hemodynamic stabilization Diagnostic
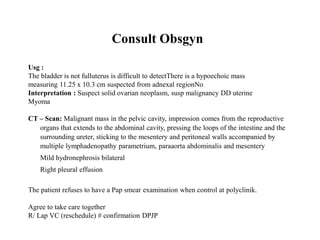
- 24. Consult Obsgyn Usg : The bladder is not fulluterus is difficult to detectThere is a hypoechoic mass measuring 11.25 x 10.3 cm suspected from adnexal regionNo Interpretation : Suspect solid ovarian neoplasm, susp malignancy DD uterine Myoma CT – Scan: Malignant mass in the pelvic cavity, impression comes from the reproductive organs that extends to the abdominal cavity, pressing the loops of the intestine and the surrounding ureter, sticking to the mesentery and peritoneal walls accompanied by multiple lymphadenopathy parametrium, paraaorta abdominalis and mesentery Mild hydronephrosis bilateral Right pleural effusion The patient refuses to have a Pap smear examination when control at polyclinik. Agree to take care together R/ Lap VC (reschedule) # confirmation DPJP
- 25. Consult Surgeon Advist: At the moment there is no treatment in our department, advice when installing intraop installation UK
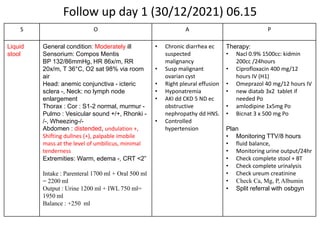
- 26. Follow up day 1 (30/12/2021) 06.15 S O A P Liquid stool General condition: Moderately ill Sensorium: Compos Mentis BP 132/86mmHg, HR 86x/m, RR 20x/m, T 36°C, O2 sat 98% via room air Head: anemic conjunctiva - icteric sclera -, Neck: no lymph node enlargement Thorax : Cor : S1-2 normal, murmur - Pulmo : Vesicular sound +/+, Rhonki - /-, Wheezing-/- Abdomen : distended, undulation +, Shifting dullnes (+), palpable imobile mass at the level of umbilicus, minimal tenderness Extremities: Warm, edema -, CRT <2” Intake : Parenteral 1700 ml + Oral 500 ml = 2200 ml Output : Urine 1200 ml + IWL 750 ml= 1950 ml Balance : +250 ml • Chronic diarrhea ec suspected malignancy • Susp malignant ovarian cyst • Right pleural effusion • Hyponatremia • AKI dd CKD 5 ND ec obstructive nephropathy dd HNS. • Controlled hypertension Therapy: • Nacl 0.9% 1500cc: kidmin 200cc /24hours • Ciprofloxacin 400 mg/12 hours IV (H1) • Omeprazol 40 mg/12 hours IV • new diatab 3x2 tablet if needed Po • amlodipine 1x5mg Po • Bicnat 3 x 500 mg Po Plan • Monitoring TTV/8 hours • fluid balance, • Monitoring urine output/24hr • Check complete stool + BT • Check complete urinalysis • Check ureum creatinine • Check Ca, Mg, P, Albumin • Split referral with osbgyn
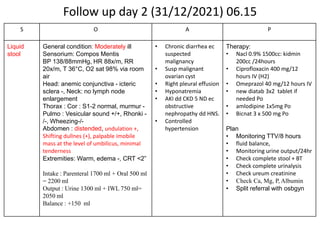
- 27. Follow up day 2 (31/12/2021) 06.15 S O A P Liquid stool General condition: Moderately ill Sensorium: Compos Mentis BP 138/88mmHg, HR 88x/m, RR 20x/m, T 36°C, O2 sat 98% via room air Head: anemic conjunctiva - icteric sclera -, Neck: no lymph node enlargement Thorax : Cor : S1-2 normal, murmur - Pulmo : Vesicular sound +/+, Rhonki - /-, Wheezing-/- Abdomen : distended, undulation +, Shifting dullnes (+), palpable imobile mass at the level of umbilicus, minimal tenderness Extremities: Warm, edema -, CRT <2” Intake : Parenteral 1700 ml + Oral 500 ml = 2200 ml Output : Urine 1300 ml + IWL 750 ml= 2050 ml Balance : +150 ml • Chronic diarrhea ec suspected malignancy • Susp malignant ovarian cyst • Right pleural effusion • Hyponatremia • AKI dd CKD 5 ND ec obstructive nephropathy dd HNS. • Controlled hypertension Therapy: • Nacl 0.9% 1500cc: kidmin 200cc /24hours • Ciprofloxacin 400 mg/12 hours IV (H2) • Omeprazol 40 mg/12 hours IV • new diatab 3x2 tablet if needed Po • amlodipine 1x5mg Po • Bicnat 3 x 500 mg Po Plan • Monitoring TTV/8 hours • fluid balance, • Monitoring urine output/24hr • Check complete stool + BT • Check complete urinalysis • Check ureum creatinine • Check Ca, Mg, P, Albumin • Split referral with osbgyn
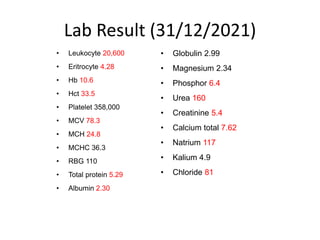
- 28. Lab Result (31/12/2021) • Leukocyte 20,600 • Eritrocyte 4.28 • Hb 10.6 • Hct 33.5 • Platelet 358,000 • MCV 78.3 • MCH 24.8 • MCHC 36.3 • RBG 110 • Total protein 5.29 • Albumin 2.30 • Globulin 2.99 • Magnesium 2.34 • Phosphor 6.4 • Urea 160 • Creatinine 5.4 • Calcium total 7.62 • Natrium 117 • Kalium 4.9 • Chloride 81
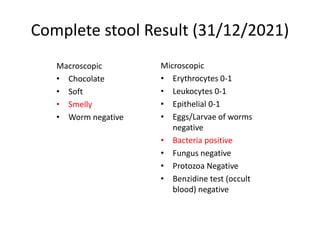
- 29. Complete stool Result (31/12/2021) Macroscopic • Chocolate • Soft • Smelly • Worm negative Microscopic • Erythrocytes 0-1 • Leukocytes 0-1 • Epithelial 0-1 • Eggs/Larvae of worms negative • Bacteria positive • Fungus negative • Protozoa Negative • Benzidine test (occult blood) negative
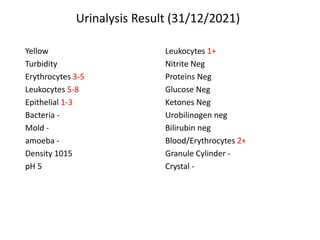
- 30. Urinalysis Result (31/12/2021) Leukocytes 1+ Nitrite Neg Proteins Neg Glucose Neg Ketones Neg Urobilinogen neg Bilirubin neg Blood/Erythrocytes 2+ Granule Cylinder - Crystal - Yellow Turbidity Erythrocytes 3-5 Leukocytes 5-8 Epithelial 1-3 Bacteria - Mold - amoeba - Density 1015 pH 5
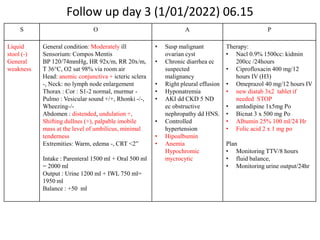
- 31. Follow up day 3 (1/01/2022) 06.15 S O A P Liquid stool (-) General weakness General condition: Moderately ill Sensorium: Compos Mentis BP 120/74mmHg, HR 92x/m, RR 20x/m, T 36°C, O2 sat 98% via room air Head: anemic conjunctiva + icteric sclera -, Neck: no lymph node enlargement Thorax : Cor : S1-2 normal, murmur - Pulmo : Vesicular sound +/+, Rhonki -/-, Wheezing-/- Abdomen : distended, undulation +, Shifting dullnes (+), palpable imobile mass at the level of umbilicus, minimal tenderness Extremities: Warm, edema -, CRT <2” Intake : Parenteral 1500 ml + Oral 500 ml = 2000 ml Output : Urine 1200 ml + IWL 750 ml= 1950 ml Balance : +50 ml • Susp malignant ovarian cyst • Chronic diarrhea ec suspected malignancy • Right pleural effusion • Hyponatremia • AKI dd CKD 5 ND ec obstructive nephropathy dd HNS. • Controlled hypertension • Hipoalbumin • Anemia Hypochromic mycrocytic Therapy: • Nacl 0.9% 1500cc: kidmin 200cc /24hours • Ciprofloxacin 400 mg/12 hours IV (H3) • Omeprazol 40 mg/12 hours IV • new diatab 3x2 tablet if needed STOP • amlodipine 1x5mg Po • Bicnat 3 x 500 mg Po • Albumin 25% 100 ml/24 Hr • Folic acid 2 x 1 mg po Plan • Monitoring TTV/8 hours • fluid balance, • Monitoring urine output/24hr
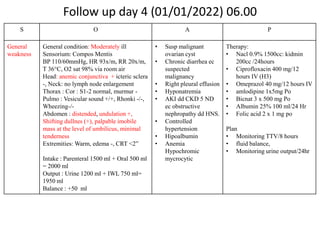
- 32. Follow up day 4 (01/01/2022) 06.00 S O A P General weakness General condition: Moderately ill Sensorium: Compos Mentis BP 110/60mmHg, HR 93x/m, RR 20x/m, T 36°C, O2 sat 98% via room air Head: anemic conjunctiva + icteric sclera -, Neck: no lymph node enlargement Thorax : Cor : S1-2 normal, murmur - Pulmo : Vesicular sound +/+, Rhonki -/-, Wheezing-/- Abdomen : distended, undulation +, Shifting dullnes (+), palpable imobile mass at the level of umbilicus, minimal tenderness Extremities: Warm, edema -, CRT <2” Intake : Parenteral 1500 ml + Oral 500 ml = 2000 ml Output : Urine 1200 ml + IWL 750 ml= 1950 ml Balance : +50 ml • Susp malignant ovarian cyst • Chronic diarrhea ec suspected malignancy • Right pleural effusion • Hyponatremia • AKI dd CKD 5 ND ec obstructive nephropathy dd HNS. • Controlled hypertension • Hipoalbumin • Anemia Hypochromic mycrocytic Therapy: • Nacl 0.9% 1500cc: kidmin 200cc /24hours • Ciprofloxacin 400 mg/12 hours IV (H3) • Omeprazol 40 mg/12 hours IV • amlodipine 1x5mg Po • Bicnat 3 x 500 mg Po • Albumin 25% 100 ml/24 Hr • Folic acid 2 x 1 mg po Plan • Monitoring TTV/8 hours • fluid balance, • Monitoring urine output/24hr
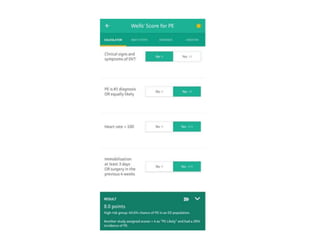
- 33. Follow up day 4 (01/01/2022) 08.22 S O A P Shortness of breath, Hemoptoe General condition: severe ill Sensorium: Compos Mentis BP 90/60mmHg, HR 118x/m, RR 24x/m, T 36°C, SPo2 85% via room air – With NRM SPO2 95 % Head: anemic conjunctiva + icteric sclera -, Neck: no lymph node enlargement Thorax : Cor : S1-2 normal, murmur - Pulmo : Vesicular sound +/+, Rhonki -/-, Wheezing-/- Abdomen : distended, undulation +, Shifting dullnes (+), palpable imobile mass at the level of umbilicus, minimal tenderness Extremities: Warm, edema -, CRT <2” PE score 8.0 – High risk group: 40.6% chance of PE • Susp malignant ovarian cyst • Chronic diarrhea ec suspected malignancy • Right pleural effusion • Hyponatremia • AKI dd CKD 5 ND ec obstructive nephropathy dd HNS. • Controlled hypertension • Hipoalbumin • Anemia Hypochromic mycrocytic • Susp. Pulmonary Emboly Therapy: • Oxygen 10 L/m via NRM • Loading fluid nacl 0.9 % 1000 cc • Ciprofloxacin 400 mg/12 hours IV (H3) • Omeprazol 40 mg/12 hours IV • amlodipine 1x5mg Po STOP • Bicnat 3 x 500 mg Po • Albumin 25% 100 ml/24 Hr • Folic acid 2 x 1 mg po Plan • Monitoring TTV/8 hours • fluid balance, • Monitoring urine output/24hr • ECG • Consult ICU • BGA
- 35. Follow up day 4 (02/01/2022) 08.25 S O A P Apnea General condition: Severely ill Sensorium: Comatose Vital signs cannot be measured and undetected Head : mydriasis pupils 3mm/3mm, Light reflex -/-, Cornea reflex -/- Thorax : No spontaneous breathing, no heartbeat Abdomen : flat Extremity: Cold EKG : asystole COD : Respiratory failure • Susp malignant ovarian cyst • Chronic diarrhea ec suspected malignancy • Right pleural effusion • Hyponatremia • AKI dd CKD 5 ND ec obstructive nephropathy dd HNS. • Controlled hypertension • Hipoalbumin • Anemia Hypochromic mycrocytic • Susp. Pulmonary Emboly • CodeBlue calls from Irina C1's room at 08.25 WITA. arrival time 08.29 WITA • performed CPR, bagging, suction and hemodynamic monitoring. • serve inj. Epinephrine 1 amp/3min. (Total administration of 2 amps of Epinephrine). • Active hematemesis (+). • Family education and ACC Intubation (Breathing aids) if ROSC and Family agree. • 08.45 am. The patient was declared dead in front of his family and medical staff.
- 37. THANK YOU
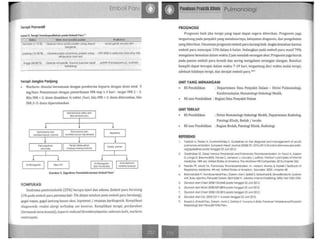
- 38. Emboli paru
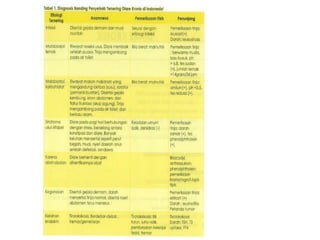
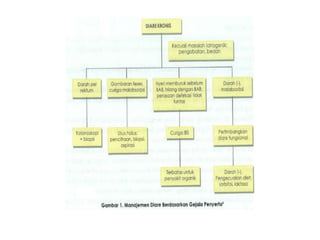
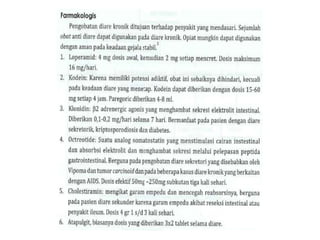
- 43. Diare kronik
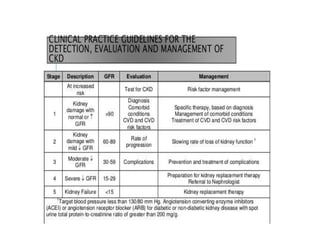
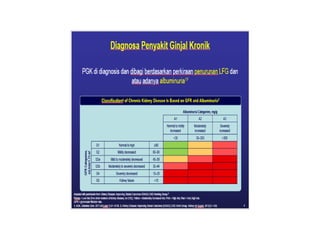
- 52. CKD
- 56. Efusi pleura
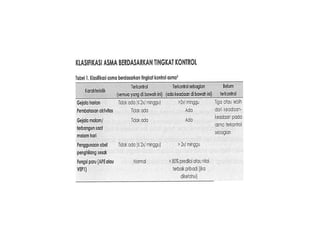
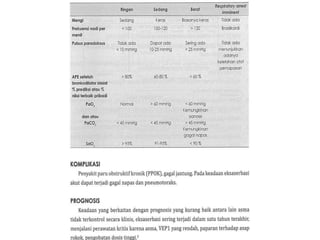
- 63. Asma
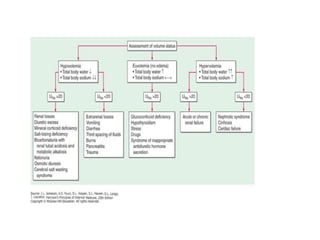
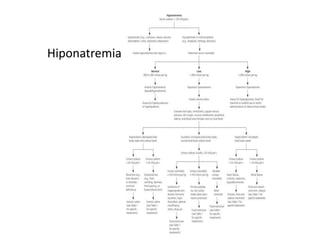
- 70. Hiponatremia
- 72. Hiponatremia