































More Related Content
What's hot (18)
Similar to Lbbb in mi (20)
















Recently uploaded (20)




















Lbbb in mi
- 1. MI IN LBBB
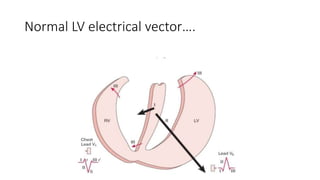
- 2. Normal LV electrical ▒╣▒│”│┘┤Ū░∙ŌĆ”.
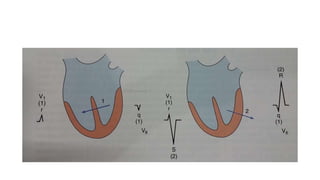
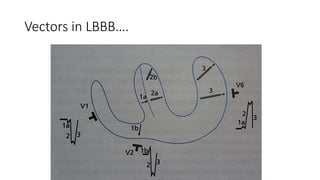
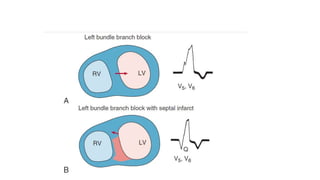
- 5. LBBBŌĆ” ŌĆó Initial septal activation with LBBB typically occurs on the right (rather than on the left) septal surface, leading to right to left (rather than left to right) activation of the septum, so that normal septal q waves are absent. ŌĆó Left ventricular activation then typically begins on the left septal surface, with a delay of 40 milliseconds or longer caused by slow transseptal spread from the right ventricular side of the septum. ŌĆó The subsequent activation of the ventricular free wall is highly variable, depending on the type, location, and extent of the underlying cardiac disease. ŌĆó Most commonly, the region of block is located anteriorly, and the lateral and posterolateral portions of the left ventricle are activated by wave fronts moving around the apex and across the inferior wall in a U-shaped pattern.
- 6. ŌĆó Irregular spread predominantly through working muscle fibers rather than the specialized conduction system results in notching and slurring of the wide QRS complex. ŌĆó Overall activation may then require more than 180 milliseconds, depending on the functional status of the distal left bundle and Purkinje systems and on the speed of propagation through working cardiac muscle; activation of portions of the left ventricle may not occur until well beyond the end of the QRS complex.
- 7. ST T CHANGES in LBBBŌĆ” ŌĆó The discordant ST-T wave pattern is a reflection of the altered pattern of ventricular activation. ŌĆó With LBBB, the right ventricle is activated and recovers earlier than the left, so recovery vectors are directed toward the right and away from the left ventricle. ŌĆó Hence positive ST-T waves will be registered in leads over the right ventricle that show S waves and negative ones over the left ventricle with prominent R waves. ŌĆó ST-T wave changes are prominent with LBBB. In most cases, the ST segment and T wave are discordant with the QRS complex. That is, the ST segment is depressed and the T wave is inverted in leads with positive QRS waves (e.g., leads I, aVL, V5, and V6), and the ST segment is elevated and the T wave is upright in leads with predominantly negative QRS complexes (e.g., leads V1 and V2). ŌĆó These ST-T wave changes are referred to secondary ST-T abnormalities because they are generated by abnormalities in conduction
- 8. ST T changes in LBBBŌĆ” ŌĆó ST-segment elevation with tall, positive T waves frequently is seen in the right precordial leads with uncomplicated LBBB. ŌĆó Secondary T wave inversions are characteristically seen in the lateral precordial leads. ŌĆó However, the appearance of ST-segment elevations in the lateral leads or ST- segment depressions or deep T wave inversions in leads V1 to V3 strongly suggests underlying ischemi. ŌĆó More marked ST-segment elevations (>0.5 mV) in leads with QS or rS waves also may be caused by acute ischemia. ŌĆó Use of the ratio of the amplitude of ST-segment elevation to S wave magnitude, determined in any relevant lead, has been proposed, with a value of less than 0.25 reported as having greater accuracy than that of the original criterion.
- 10. Electromechanical dissociation. ŌĆó Septal and lateral wall moves in dys synchrony. ŌĆó More than 60 msec of dyssynchrony is commom and as much as 120 to 150 msec out of phase contractions can occur between lateral and septal wall.
- 11. ŌĆóMI IN LBBB
- 12. The diagnosis of myocardial infarction may be obscured ŌĆó LBBB can mask or mimic MI. ŌĆó emergence of abnormal Q waves with infarction is dependent on a normal initial sequence of ventricular activation, which is absent with LBBB. ŌĆó In addition, ECG patterns of LBBB, including low R wave amplitude in the midprecordial leads and ST-T wave changes, can mimic anterior infarct patterns.
- 13. ŌĆó The diagnosis of infarction in the presence of LBBB is considerably more complicated and confusing, because LBBB alters the early and the late phases of ventricular depolarization and produces secondary ST-T changes. ŌĆó These changes may mask and/or mimic myocardial infarction findings. ŌĆó Infarction of the left ventricular free (or lateral) wall ordinarily results in abnormal Q waves in the midprecordial to lateral precordial leads (and selected limb leads). ŌĆó However, the initial septal depolarization forces with LBBB are directed from right to left. These leftward forces produce an initial R wave in the midprecordial to lateraprecordial leads, usually masking the loss of electrical potential (Q waves) caused by the infarction. ŌĆó Thereforeacute or chronic left ventricular free wall infarction by itself will not produce diagnostic Q waves in the presence of LBBB
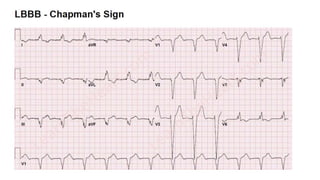
- 14. Hard signs of MI in LBBBŌĆ” ŌĆó The presence of QR complexes in leads I, V5, or V6 or in II, III, and avf with LBBB strongly suggests underlying infarction. ŌĆó Chronic infarction also is suggested by notching of the ascending part of a wide S wave in the midprecordial leads or the ascending of a wide R wave in lead I, aVL, V5, or V6.
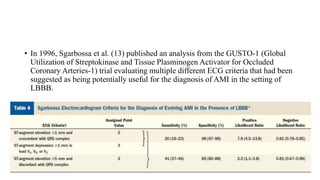
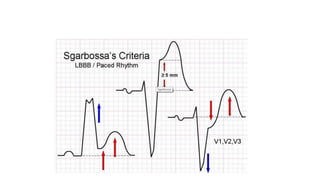
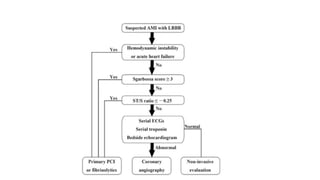
- 16. ŌĆó In 1996, Sgarbossa et al. (13) published an analysis from the GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries-1) trial evaluating multiple different ECG criteria that had been suggested as being potentially useful for the diagnosis of AMI in the setting of LBBB.
- 18. SMITH modification of Sgarbossa criteriaŌĆ” ŌĆó A new criterion from Smith et al. significantly increases the sensitivity (up to 90%) ŌĆó ST elevation or depression in the opposite direction as the QRS with a ST/S ratio of ŌłÆ0.25 or less (ie that the ST deviation is bigger than 25% of the S wave amplitude) In summary ŌĆó All those criteria can be put together like this: ŌĆó ST deviation ŌĆó ŌĆō Ōēź0.1 mV in the same direction as the QRS or ŌĆó ŌĆō ST/S ratio Ōēź 25%
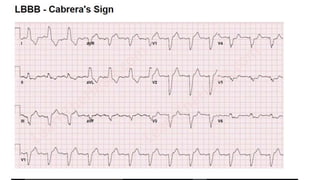
- 19. ŌĆó Cabrera's sign ŌĆó CabreraŌĆÖs sign is used to diagnose an acute myocardial infarction in the setting of a left bundle branch block and consists of notching at 40 milliseconds in the upslope of the S wave in lead V3 and V4. This has a poor sensitivity of 27% for myocardial infarction
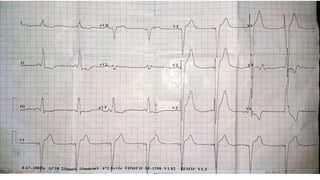
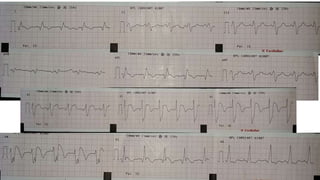
- 22. ŌĆó Mohammad kunju 65/m ŌĆó Known case of CAD, DCM, HTN ŌĆó MI 4 years back. ŌĆó ED III for 4 months. ŌĆó Elective PCI to prox LAD 3 months back. ŌĆó Presented with chest pain.. ŌĆó ECG was taken.
- 26. Refrences.. ŌĆó Braunwalds text book of Heart Diseases 10th edition. ŌĆó Leo scamroth ,An introduction to Electrocardiography 8th edi. ŌĆó Evolving Considerations in the Management of Patients With Left Bundle Branch Block and Suspected Myocardial Infarction JACC Vol. 60, No. 2, 2012 Neeland et al. 99 July 10, 2012:96ŌĆō10 ŌĆó Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Smith et al Ann Emer Med 2012 Dec;60(6):766-76