


























































![Fungal infections of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/fungalinfectionsofskincompatibilitymode-130321223403-phpapp01-thumbnail.jpg?width=560&fit=bounds)












More Related Content
What's hot (20)
Similar to Lichen planus (20)


















Recently uploaded (20)












Lichen planus
- 1. LICHEN PLANUS By- Dr. Shweta Khushalani ( JR-1, Dept. Skin & V.D.)
- 2. Introduction Idiopathic, chronic, inflammatory disease that affects the skin, mucous membranes and appendages. History âLeichenâ = tree moss âPlanusâ = flat Lichen planus = Eramus Wilson,1869 Wickhamâs striae = Wickham, 1895
- 3. Epidemiology ïž0.1% - 4% ïž> 45 years of age ïžWomen > men ïžChild : 1-4% of cases of LP; family history significant.
- 4. Etiopathogenesis âĒ Unknown, ?AUTOIMMUNE âĒ ETIOLOGY : â Idiopathic. â Drugs. â Infections & vaccination. â Associated with autoimmune disorders. â Contact allergens â Mechanical trauma âĒ Genetic association : HLA- A3, BW35, B8, B16, DR1, DQW1
- 5. Drugs âĒ Heavy metals âĒ Antimalarials âĒ Antibiotics âĒ AKT âĒ Diuretics âĒ Antihypertensives âĒ Anticonvulsant âĒ NSAIDS âĒ Oral hypoglycemics âĒ Antihistaminics âĒ Lipid lowering agents âĒ Miscellaneous Autoimmune disorders âĒ Ulcerative collitis âĒ Type 2 DM âĒ Myasthenia gravis âĒ Lupus erythematous âĒ Alopecia aerata Infections & vaccination âĒ Hepatitis B & C âĒ Influenza âĒ MMR âĒ DPT
- 6. âĒ Antigen specific & nonspecific killing by t- lymphocytes ( both helper & supressor cells) âĒ Th17 play imporatnt role, secrete IL-17 âĒ IL-17 upregulate and/or synergize with local inflammatory mediators and extracellular matrix injury by MMP (matrix metallo- protienases) âĒ Other cytokines- â TNF-alpha, â Nuclear factor-Kbeta dependent cytokines â IFN-gamma â IL-1alpha, IL-6, IL-8
- 7. Clinical features âĒ Extremely pruritic âĒ Flat topped âĒ Polygonal âĒ Violaceous papules or plaques âĒ 3-15mm in diameter âĒ Wickhamâs striae â â delicate, radiating, white scales â Focal thickening of granular layer âĒ Positive Koebnerâs phenomenon
- 8. âĒ Sites : â Flexors surfaces of forearm & wrist, dorsal surface of hands â Anterior aspect of lower legs, neck, lower back. â Heal with hyperpigmentation.
- 9. Histology
- 10. Lichen Planus Verrucosus âĒ K/a Hypertrophic LP âĒ Extremely pruritic âĒ Hyperkeratotic plaques on the shin and ankles âĒ Can transform into metastatic squamous cell carcinoma (esp. distal extremeties)
- 11. Atrophic Lichen Planus âĒ Lower limbs âĒ Violaceous papules and plaques with depressed and atropic center âĒ Usually occurs after resolution of typical LP & Accentuate by potent topical steroids
- 13. Annular LP âĒ Glans & trunk âĒ Typical violaceous papules, in a ring like fashion âĒ Central clearing leaving behind active raised border âĒ Variant : AALP ( Annular Atrophic LP) â Small violaceous papules â Slowly grow peripherally â Center:atrophic and hyperpigmented â Peripherally raised â Trunk, limbs
- 14. Linear LP âĒ Spontaneous âĒ Linear along Lines of Blaschko âĒ children > adults âĒ Rarely, occur at the site of healed herpes zoster scar
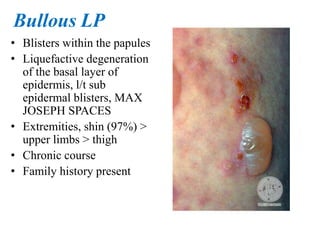
- 15. Bullous LP âĒ Blisters within the papules âĒ Liquefactive degeneration of the basal layer of epidermis, l/t sub epidermal blisters, MAX JOSEPH SPACES âĒ Extremities, shin (97%) > upper limbs > thigh âĒ Chronic course âĒ Family history present
- 17. LP Pemphigoides âĒ Blisters on LP lesions + non affected skin âĒ Distal limbs âĒ Histology âĒ Direct Immunofluorescence Deposition of IgG & C3 at BMZ
- 19. Actinic LP âĒ Summer months âĒ Sun exposed areas, forehead and face, dorsal surface of hands and neck âĒ Blue, brownish plaque, annular hypopigmented border with central atrophy âĒ Young adults & children âĒ NO PRURITIS âĒ NO KOEBNERIZATION
- 20. LP Pigmentosus âĒ Slate grey to brownish- black macules âĒ sun exposed areas & flexural folds âĒ Types â Diffuse (most common) â Blotchy â Reticular â Perifollicular
- 21. Lichen Planopilaris âĒ a/k/a Follicular LP âĒ Chronic lymphocytic inflammation around the upper portion of hair follicle âĒ Irregular patchy loss of hair, with loss of follicular ostia. âĒ Multifocal, patchy > diffuse âĒ Perifollicular erythema and scaling + on periphery of the lesion âĒ Disease activity, periphery>center of the alopecia patch âĒ Pruritis with dysesthesia âĒ Site â frontocentral scalp & crown
- 22. âĒ 50% a/w typical LP lesions over non-follicular skin, nail, mucous membrane
- 24. Erosive LP âĒ Mucosal surface âĒ Oral cavity or genitalia âĒ Erosions on the surface of papular lesions âĒ Aggressive form of LP Eruptive LP âĒ A/k/a acute or exanthematous LP âĒ Disseminated form âĒ Trunk, dorsum of feet & wrist âĒ Self-limiting âĒ Heal in 3-9months with hyperpigmentation.
- 25. Nail LP âĒ 10% âĒ Finger nails>toe nails âĒ Adults ( 50-60 years ) âĒ In pediatric age , nail LP>skin LP âĒ Chronic course âĒ 3 presentations â Typical Nail LP â Twenty Nail Dystrophy (trachyonychia) â Idiopathic Atrophy of Nails
- 26. TYPICAL NAIL LP âĒ diffuse nail ridging âĒ splitting âĒ dorsal pterygium TWENTY NAIL DYSTROPHY âĒ Excessive longitudnal ridging l/t nail roughness âĒ Beningn condition âĒ No nail scarring âĒ One to several nails affected IDIOPATHIC ATROPHY OF THE NAIL âĒ acute & rapid, painless, destruction of the nail OTHERS âĒ Yellow nail syndrome like changes âĒ Nail bed erosions âĒ Pigmentary changes : longitudnal melanonychia, longitudnal erythronychia
- 28. TYPICAL NAIL LP âĒ diffuse nail ridging âĒ splitting âĒ dorsal pterygium TWENTY NAIL DYSTROPHY âĒ Excessive longitudnal ridging l/t nail roughness âĒ Beningn condition âĒ No nail scarring âĒ One to several nails affected IDIOPATHIC ATROPHY OF THE NAIL âĒ acute & rapid, painless, destruction of the nail OTHERS âĒ Yellow nail syndrome like changes âĒ Nail bed erosions âĒ Pigmentary changes : longitudnal melanonychia, longitudnal erythronychia
- 30. TYPICAL NAIL LP âĒ diffuse nail ridging âĒ splitting âĒ dorsal pterygium TWENTY NAIL DYSTROPHY âĒ Excessive longitudnal ridging l/t nail roughness âĒ Beningn condition âĒ No nail scarring âĒ One to several nails affected IDIOPATHIC ATROPHY OF THE NAIL âĒ acute & rapid, painless, destruction of the nail OTHERS âĒ Yellow nail syndrome like changes âĒ Nail bed erosions âĒ Pigmentary changes : longitudnal melanonychia, longitudnal erythronychia
- 32. Palmoplantar LP âĒ Rare âĒ Highly pruritic, erythematous, scaly plaque with/out plamoplantar keratoderma âĒ Internal plantar arch & hands (NO FINGERTIPS) âĒ Young adults (20-40 years age)
- 33. Oral LP âĒ In 70-77% of cutaneous disease âĒ 25% present with oral LP âĒ Middle age (40-70 years), women âĒ 6 types (ANDREASEN CLASSIFICATION) â RETICULAR â PLAQUE-LIKE â PAPULAR â EROSIVE â ATROPHIC â BULLOUS âĒ Lateral margins of tongue, gingiva, lips and hard palate âĒ Chronic course âĒ STRESS, SPICY & ACIDIC FOOD- flare up âĒ Association with HCV infection âĒ Risk of malignant transformation in 0.4-1.5%
- 34. RETICULAR LP âĒ Most common âĒ Asymptomatic âĒ Irregular patchy, plaque with white streaks in a lacy pattern âĒ posterior buccal mucosa âĒ Bilateral EROSIVE ORAL LP âĒ Large, erythematous, well defines erosions on buccal mucosa âĒ with/out pseudomembrane âĒ Buccal mucosa, Dorsum & lateral borders of tongue, gingiva ATROPHIC LP âĒ Gingiva âĒ Irritaion following eating & brushing
- 36. Genital LP âĒ 25% cases with skin LP âĒ Males â Shaft of penis, glans penis, prepuce, scrotum â ANNNULAR LP (most common presentation)
- 37. âĒ Female â Vulval and vaginal â Vulval : on introitus, white lacy, reticular borders extending into vagina â Dyspareunia â a/w pruritis and pain â Loss of normal architecture and scarring on healing âĒ VVG (VULVO-VAGINAL-GINGIVAL) SYNDROME â Erosive lesions â a/w HLA-DQB1*0201 allele
- 38. Esophageal LP âĒ Rare âĒ Middle age, women, with oral LP âĒ c/o dysphagia, odynophagia, or both âĒ Endoscopy âĒ Strictures & malignant transformation to Squamous cell carcinoma common
- 39. Complications âĒ Hyperpigmentation âĒ NAIL LP : dystrophy of nail, anonychia âĒ LPP SCALP : scarring alopecia âĒ GENERALISED LP : erythroderma âĒ ULCERATIVE LP ON FEET : deformity âĒ HYPERTROPHIC & MUCOSAL LP : malignant transformation
- 40. Treatment FIRST LINE â Topical corticosteroids â First generation antihistaminics (hydroxyzine / chloprpheniramine) â Intra-lesional steroids (hypertrophic , nail & erosive LP) â Immunomodulator (tacrolimus, pacrolimus) â Topical minoxidil (LPP)
- 41. SECOND LINE â Systemic corticosteroids (oral or IM) â Oral prednisolone : 0.5-1mg/kg/day for 4-6 weeks â Oral mini pulse with betamethsone â IM inj. Of Triamcinolone :40-80mg, every 6-8 weeks â Phototherapy âĒ NB-UVB âĒ PUVA âĒ Extracorporeal photopheresis, in recalcitrant & severe erosive LP
- 42. THIRD LINE â Immunosupressive agents : âĒ azathioprine, âĒ Methotrexate ( 10-15mg/week, severe erosive & generalised LP) âĒ Cyclophosphamide âĒ Cyclosporine (severe resistant cutaneous LP & LPP) âĒ Mycophenolate mofetil â Hydroxychloroquine : LPP â Others âĒ Dapsone âĒ IFN-alpha âĒ Isotretenion âĒ Thalidomide âĒ sulfasalazine
- 43. MUCOSAL LP â First line : Topical steroids âĒ Intralesional steroids used in localised ulcerative LP âĒ Local phototherapy : NB-UVB and PUVA âĒ excimer 308 nm laser with ECP in recalcitrant oral LP â Second line : âĒ Systemic corticosteroids , short term âĒ Hydroxycholoroquine
- 44. THANKYOU