


























![benign neck disease [Autosaved].pptx orlhns](https://cdn.slidesharecdn.com/ss_thumbnails/benignneckdiseaseautosaved-241117151930-f0f5c123-thumbnail.jpg?width=560&fit=bounds)


















More Related Content
Similar to Meningioma presentation by dr,Mumtaz Ali narejo (20)
More from Neurosurgeon Mumtaz Ali Narejo (20)


















Recently uploaded (20)




















Meningioma presentation by dr,Mumtaz Ali narejo
- 1. MENINGIOMA DR.MUMTAZ ALI NAREJO CONSULTANT NEUROSPINE & CEREBROVASCULAR SURGEON
- 2. OUTLINES ? Main features ? Common location ? Investigations ? Types ? Sindou et All ? Surgical principles ? Simpson grading ? Histopathological grading ? Recurrence rate ? Radiotherapy
- 3. Main Features ? Most common primary intracranial tumors ? Extra-axial ? F:M = 1.8:1 ? Mean age : 45 years ? usually slow growing ? circumscribed (non-infiltrating) ? benign lesions ? arachnoid cap cells (meningothelial cells) ? Ectopic meningiomas ? Psammoma bodies
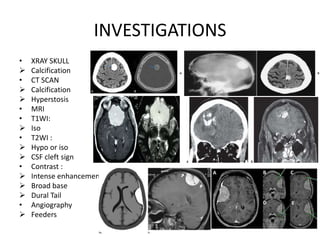
- 5. INVESTIGATIONS ? XRAY SKULL ? Calcification ? CT SCAN ? Calcification ? Hyperstosis ? MRI ? T1WI: ? Iso ? T2WI : ? Hypo or iso ? CSF cleft sign ? Contrast : ? Intense enhancement ? Broad base ? Dural Tail ? Angiography ? Feeders
- 7. TYPES ; SPHENOID WING ? lateral sphenoid wing (or pterional): ? Middle third (or alar) ? Medial (clinoidal): ?ICA ?MCA ?cranial nerves ?optic nerve ?compress brainstem ?Total removal is often not possible ?Pterional craniotomy
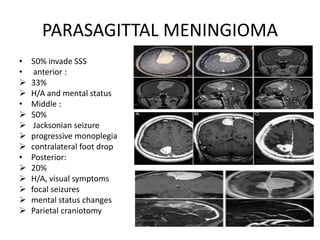
- 8. PARASAGITTAL MENINGIOMA ? 50% invade SSS ? anterior : ? 33% ? H/A and mental status ? Middle : ? 50% ? Jacksonian seizure ? progressive monoplegia ? contralateral foot drop ? Posterior: ? 20% ? H/A, visual symptoms ? focal seizures ? mental status changes ? Parietal craniotomy
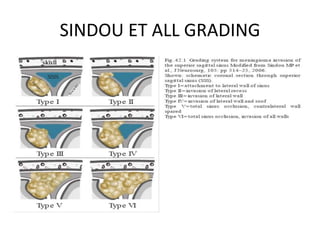
- 9. SINDOU ET ALL GRADING
- 10. OLFACTORY GROOVE MENINGIOMA ? Foster Kennedy syndrome ? Anosmia ? ipsilateral optic atrophy ? contralateral papilledema ? Mental status changes ? frontal lobe findings ? Apathy & Abulia ? urinary incontinence ? optic apparatus ? visual impairment ? fornix ? short-term memory loss ? seizure ? Bifrontal craniotomy ? Subfrontal Approach
- 11. PLANUM SPHENOIDALE & TUBERCUM SELLA MENINGIOMA
- 12. FORAMEN MAGNUM MENINGIOMA ? Anterior : 31% ? Lateral : 56% ? Posterior : 13%
- 13. CONVEXITY MENINGIOMA ? Pre-coronal ? Coronal ? Post-coronal
- 17. SURGERY : PRINCIPLE ? Preoperative embolization ? Autologous blood donation ? Early interruption of the blood supply ? Internal decompression ? Dissection of the tumor capsule ? Removal of attached bone & dura
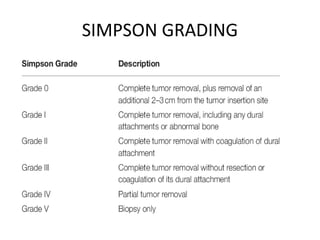
- 18. SIMPSON GRADING
- 20. RADIOTHERAPY ? RECURRENCE RATE : 5¨C15 years ? total resection : 4 % ? partial resection without XRT : 60% ? partial resection with XRT : 32%
- 21. THANKYOU