



































Monteggia fracture in children
- 1. Antibiotics Protocols in orthopedics Dr Razi Ullah Resident orthopedics Surgeon ATH
- 2. ŌĆó Infection in orthopedic surgery is one of the most dreaded complications. ŌĆó It is associated with prolonged morbidity, disability and increased mortality. ŌĆó Out of nearly 30 million operations in the United States each year more than 2% are complicated with surgical site infections. ŌĆó The mortality rate increases 2ŌĆō3 times after infection.
- 3. ŌĆó Antibiotics are the cornerstone of prevention and management of orthopedics infection. ŌĆó We will discuss protocols of antibiotics in ŌĆó 1. Open fractures ŌĆó 2.Surgical prophylaxis ŌĆó 3. Bone infection
- 4. ŌĆó Protocol of Antibiotics in open fractures ŌĆó Gustilo type 1 and 2 ŌĆó First generation cephalosporin for 24 hours ŌĆó Type 3A ŌĆó First generation cephalosporin plus a aminoglycoside since 72 hours since last incision and drainage ŌĆó Type 3B highly contaminated farm injuries ŌĆó First generation cephalosporin plus aminoglycoside plus high dose penicillin 72 hours since last incision and drainage
- 5. ŌĆó Freshwater wounds ŌĆó Flouroquinolones or third or fourth generation cephalosporin ŌĆó Saltwater wounds ŌĆó Doxycycline and fourth generation cephalosporin or flouroqunolones
- 6. ŌĆó Protocol for Surgical prophylaxis ŌĆó There is enough evidence to say that prophylactic antibiotics should be used in orthopedics to reduce surgical site infection ŌĆó We will discuss timing,choice and duration of antibiotics for prophylaxis in surgical patients
- 7. ŌĆó Timing of administration ŌĆó The timing of administration remains controversial. ŌĆó Evidence shows that initiating prophylaxis after the skin is incised, is ineffective. ŌĆó Most of the studies agree that prophylactic antibiotics should ideally be administered 30ŌĆō60 min before skin incision ŌĆó Administration >60 min before surgery/incision is associated with higher risk of surgical infections
- 8. ŌĆó The prophylaxis has least effect when antibiotic is given after the application of a tourniquet
- 9. ŌĆó Which antibiotics? The antibiotic selected should in general, be inexpensive, nontoxic and of limited spectrum. The most prevalent organisms in prosthetic related infections are Gram-positive Staphylococcus aureus and epidermidis
- 10. ŌĆó According to American Society of Health System Pharmacists (ASHP) cefazolin was the most used antibiotic in preoperative prophylaxis, combination of cefazolin with gentamicin was the second common regimen while 3rd generation cephalosporin were 3rd widely used antibiotics.
- 11. ŌĆó In a study, 3rd generation cephalosporins were most commonly used for arthroplasty prophylaxis and 2nd generation cepholospirins were used for fracture fixation.
- 12. ŌĆó Duration of antibiotics ŌĆó The controversy persists in administration of antibiotics varying from a single dose to 3 doses to 5 days or 14 days ŌĆó The ideal duration of postoperative antibiotics is not yet clearly defined although most reports say that there is no additional benefit when prophylactic antibiotics are given more than 24 h postsurgery
- 13. ŌĆó Musmar et al. suggests that antibiotics should be discontinued within 24 h after end of surgery to prevent emergence of resistance ŌĆó Thonse et al. recommended prophylactic antibiotic regimen at time of induction of anesthesia and two subsequent doses at 8 and 16 h postoperatively. ŌĆó Another study by Andersson et al. suggest same recommendations of 3 doses within 24 h.
- 14. ŌĆó Niimi et al. in a retrospective study compared the outcome of 1-day intravenous administration with that of long term intravenous administration in arthroplasty cases. They used antibiotics for 1-day (n = 233) and for at least 3 days (n = 104) ŌĆó None of these patients developed wound infection during follow up (minimum 12 months). ŌĆó They concluded that 1-day antibiotic infusion was as effective as long term antibiotic infusion preventing infection after arthroplasty.
- 15. ŌĆó Protocol of antibiotics in osteomyelitis ŌĆó Empirical antibiotics ŌĆó Coverage for the most likely infecting organism should be started till gram stain results appear or if negative. ŌĆó Recommendations for the initiation of empiric antibiotic (according to age of the patient and mechanism of infection
- 16. ŌĆó Hematogenous osteomyelitis ( newborn to adult combination of penicillinase-resistant synthetic penicillin (Oxacillin or nafcillin) +third-generation cephalosporin. ŌĆó MRSA ŌĆó vancomycin or clindamycin +third-generation cephalosporin, Linezolid is also used in these circumstances.
- 17. ŌĆó Sickle cell disease:S aureus and Salmonellae species-- ----fluoroquinolone antibiotic (not in children). ŌĆó A third-generation cephalosporin (eg, ceftriaxone) is an alternative choice ŌĆó In diabetic foot----S aureus and Pseudomonas aeruginosa----ceftazidime or cefepime. Ciprofloxacin is an alternative treatment.
- 18. ŌĆó Prosthesis infections S epidermidis----biofilm---- protect bacteria against phagocytosisd antibiotics. Rifampicin: Must be used in combination with other antibiotics because it acts on the biofilm and avoids recurrence if used within a month of treatment
- 19. Start IV: The response to appropriate IV antibiotic usually occur in 48 hr Lack of improvement in fever and pain after this ----- surgical drainage. Then use IV (according to culture) for 2 weeks Oral (combination) for 4 weeks --(revascularization of bone takes 4 weeks
- 20. ŌĆó Duration of antibiotic therapy ŌĆó Most infections- eg S. aureus, a total of 6 wk. ŌĆó For group A streptococcus, S. pneumoniae, or H. influenzae type b---, shorter. ŌĆó Immunocompromised patients, mycobacterial or fungal infection ---- prolonged courses of therapy.
- 22. ŌĆó Radial head dislocation plus proximal ulna fracture or ŌĆó Plastic deformation of the ulna without obvious fracture ŌĆó Peak age is 4-10 years in children
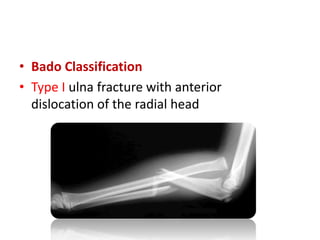
- 24. ŌĆó Bado Classification ŌĆó Type I ulna fracture with anterior dislocation of the radial head
- 25. ŌĆó Type II proximal ulna fracture with posterior dislocation of the radial head
- 26. ŌĆó Type III proximal ulna fracture with lateral dislocation of the radial head
- 27. ŌĆó Type IV Fractures of both the radius and ulna at the same level with an anterior dislocation of the radial head (1-11% of cases)
- 28. ŌĆó Monteggia equivalents ŌĆó isolated radial head dislocation with plastic deformity of ulna ŌĆó fracture of the proximal ulna with fracture of the radial neck, and ŌĆó Both bone proximal third fractures with the radial fracture more proximal than the ulnar fracture
- 29. ŌĆó Imaging ŌĆó Obtain standard AP and lateral views ŌĆó Assess radiocapitellar line on every lateral radiograph of the elbow ŌĆó A line down the radial shaft should pass through the center of the capitellar ossification center in all elbow positions
- 32. ŌĆó Treatment closed reduction of ulna and radial head dislocation and long arm casting Indicated for BADO I-III when 1.Radial head is stable following reductions 2. Length stable ulnar fracture pattern
- 33. ŌĆó Radial head will reduce spontaneously with reduction of the ulna and restoration of ulnar length ŌĆó Patients should be immobilized in a long arm cast in 90 to 100 degrees of flexion and supination and followed closely radiographically for 2 to 3 weeks to ensure maintenance of radial head reduction.
- 34. ŌĆó Operative ŌĆó Plating of ulna + reduction of radial head ┬▒ annular ligament repair/reconstruction ŌĆó Indication ŌĆó Bado Types I-III with radial head is not stable following reduction ulnar length is not stable (unable to maintain ulnar length) ŌĆó acute Bado Type IV ŌĆó open fractures ŌĆó older patients Ōēź 10y if closed reduction is not stable
- 35. ŌĆó Technique ŌĆó Annular ligament reconstruction almost never required for acute fractures ŌĆó open reduction of radial head through a lateral approach if needed in chronic (>2-3 weeks old) Monteggia fractures where radial head still retains concave structure ŌĆó Chronic Monteggia requires ulnar osteotomy with annular ligament reconstruction via triceps tendon harvesting
- 37. ŌĆó Complications ŌĆó posterior interosseous nerve neuropraxia (10% of acute injuries)almost always spontaneously resolves ŌĆó Delayed or missed diagnosis is common when evaluation not performed by an orthopaedic surgeon ŌĆó complication rates and severity increase if diagnosis delayed >2-3 weeks
- 38. Thank You