Muscle Energy Technique
?Download as PPTX, PDF?
15 likes?4,100 views

This document discusses muscle energy technique (MET), a manual therapy procedure that involves voluntary muscle contraction against resistance applied by a therapist. It describes the types of muscle contractions involved - isotonic, eccentric, concentric, and isometric. MET uses post-isometric relaxation and reciprocal inhibition to facilitate muscle lengthening. Indications for MET include acute muscle spasm and restricted joints, while contraindications are acute injuries and unstable joints. Benefits of MET include restoring normal muscle tone, strengthening weak muscles, and improved joint mobility. Guidelines are provided for safely applying light contractions over multiple repetitions.


Muscle Energy Technique
- 1. Muscle Energy Technique ? Dr Shrikrishna Shinde Assistant professor at MVPS College of Physiotherapy Nashik
- 2. Objectives Muscle energy technique Types of muscle contraction. Principles of MET Techniques of application Indications, contraindication of MET. Benefits of MET.
- 3. MUSCLE ENERGY TECHNIQUE Muscle energy technique is a manual therapy procedure which involves the voluntary contraction of a muscle in a precisely controlled direction at varying levels of intensity against a distinct counter force applied by the therapist.
- 4. Types of Contraction Types of Contraction Isotonic contraction Eccentric contraction- Concentric contraction- Isometric contraction
- 5. Types of Contraction Isometric contraction Isotonic contraction
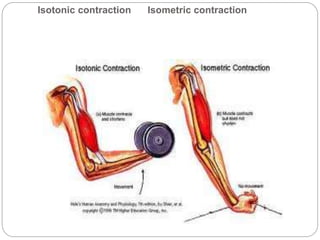
- 6. Isotonic contraction Isometric contraction
- 7. It is a type of muscle contraction in which the muscles shorten while generating force. This occurs when the force generated by the muscle exceeds the load opposing its contraction the muscle elongates while under tension due to an opposing force greater than the muscle force. Concentric contraction- Eccentric contraction-
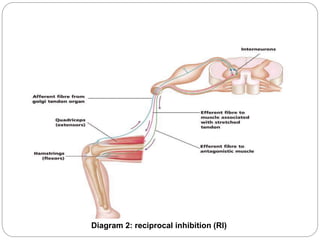
- 9. ? When an agonist muscle contracts and shortens, its antagonist must relax and lengthen so that motion can occur under the influence of the agonist muscle. ? The contraction of the agonist reciprocally inhibits its antagonist allowing smooth motion. ? The harder the agonist contracts, the more inhibition in the antagonist, causing relaxation Reciprocal inhibition
- 10. Diagram 2: reciprocal inhibition (RI)
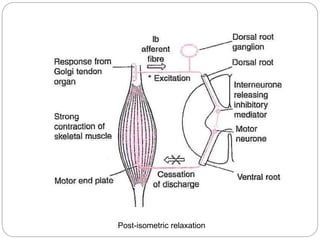
- 11. ? Post Isometric Relaxation
- 13. APPLICATION OF THE TECHNIQUES Isotonic contraction using Post-Isometric Relaxation Isotonic contraction using Reciprocal Inhibition
- 14. ? Indication ĻC 1.acute muscular spasm or 2.to mobilise a restricted joint ? Procedure - The therapist takes the agonist muscle to its barrier position; then ask the patient to contract muscle then therapist apply equal resistance to the patients contracting the agonist muscle , for 7-10 seconds. Patient relaxes for around 5 seconds, and then as they exhale, the therapist takes muscle to the new restriction barrier, and the process is repeated 3 to 5 times. Isotonic contraction using Post-Isometric Relaxation
- 15. ? Indication -condition of chronic, fibrotic muscular spasm. ? In this tech. we have to apply same procedure as PIR. The difference is that we have to target antagonistic muscle. Isotonic contraction using Reciprocal Inhibition
- 16. ? Lengthen shortened, contracted muscle. ? Spasticity. ? Strengthen weak muscle or group of muscles. Indications of MET:
- 17. ? Acute musculoskeletal injuries ? Unset or unstable fracture ? Unstable or fused joints Contraindications of MET:
- 18. ? Restoring normal tone in hypertonic muscles. ? Strengthening weak muscles. ? Preparing muscle for subsequent stretching. ? Improved joint mobility. The benefits of MET
- 19. ? No pain should be caused by MET. ? Keep contractions light (20-30% of strength) ? Communicate effectively and ensure client is not experiencing discomfort. ? Never over-stretch. Simple guidelines for using MET:
- 20. ? Chaitow L. Muscle Energy Techniques. 3rd ed. Philadelphia: Churchill Livingstone Elsevier2006. 3.ternal operf the muscle ? Matthews PB. Evolving views on the ination and functional role ol. Nov 1981;320:1Đ\30. 4.sibility. Phy820. ? spindle. J Physiosiol Rev. Oct 1978;58(4):763Đ\5.y. 7th ed: WB Saunders; 1986. ? McCloskey DI. Kinesthetic sen Guyton A. Textbook of Medical Physiolog6. ? Denegar C, Saliba S, Saliba E. Therapuetic Modalities for Musculoskeletal Injuries. 2nd ed. Champaign, IL: Human Kinetics; 2006. 7. Weng MC, Lee CL, Chen CH, et al. Effects of different stretching techniques on the outcomes ? of isokinetic exercise in patients with knee osteoarthritis. Kaohsiung J Med Sci. Jun 2009;25(6):306Đ\315. 8.AM, Schwartz SL, et al. A randomizedour techniques. J Strength Con ? Fasen JM, O'Connor controlled trial of hamstring stretching: comparison of fd Res. Mar 2009;23(2):660Đ\667. 9. ? Ward RC, Hruby RJ. Foundations for Osteopathic Medicine. 2nd ed. Philadelphia: Lippencott Williams & Wilkins; 2002. 10. flexibility of ? Smith M, Fryer G. A comparison of two muscle energy techniques for increasingthe hamstring muscle group. J Bodyw Mov Ther. Oct 2008;12(4):312Đ\317. 11. Mahieu NN, Cools A, De Wilde B, Boon M, Witvrouw E. Effect of proprioceptive References
- 21. ? 12. Christensen BK, Nordstrom BJ. The effects of proprioceptive neuromuscular facilitation and ? dynamic stretching techniques on vertical jump performance. J Strength Cond Res. Nov2008;22(6):1826Đ\1831. 13. Kofotolis N, Kellis E. Effects of two 4Đ\week proprioceptive neuromuscular facilitation ? programs on muscle endurance, flexibility, and functional performance in women with chronic low back pain. Phys Ther. Jul 2006;86(7):1001Đ\1012. 14.ing : ? Sharman MJ, Cresswell AG, Riek S. Proprioceptive neuromuscular facilitation stretchmechanisms and clinical implications. Sports Med. 2006;36(11):929Đ\939. 15. Caplan N, Rogers R, Parr MK, Hayes PR. The effect of proprioceptive neuromuscular Res. Jul ? facilitation and static stretch training on running mechanics. J Strength Cond2009;23(4):1175Đ\1180. 16.Đ\ ? Atchison JW. Manipulation for the treatment of occupational low back pain. Occup Med. JanMar 1998;13(1):185Đ\197. 17. Burns DK, Wells MR. Gross range of motion in the cervical spine: the effects of osteopathic ? muscle energy technique in asymptomatic