












![? Physician, A.F. (2001) American Family Physician, 1
October, [Online], Available:
http://www.aafp.org/afp/2001/1001/p1261.html
[16 August 2013].
? Early prevention of left ventricular dysfunction after
myocardial infarction with angiotensin-converting-
enzyme inhibition
?
The Lancet, Volume 337, Issue 8746, Pages 872-876
N Sharpe, H Smith, J Murphy, S Greaves, H Hart, G
Gamble
? Ribeiro, A. L. et al. (2012) Diagnosis and management
of Chagas disease and cardiomyopathy Nat. Rev.
Cardiol. doi:10.1038/nrcardio.2012.109](https://image.slidesharecdn.com/establishedmyocardialinfarction-150630203027-lva1-app6892/85/Myocardial-infarction-16-320.jpg)
Myocardial infarction
- 2. ? 18/07/2013 48 y/o Indian Male came to casualty at 20:40 C/O sub-sternal chest pain, radiating to left arm, SOB and paresthesia since 13:00.
- 3. ? ~8 hours ago, chest pain, radiating to the left, paresthesia in the left arm and shortness of breath, diaphoresis. He was resting at home. ? MVA 2012, injury to R arm ? No other Hx ? Smokes +-20 cigarettes a day, diet, family Hx
- 4. ? Pt in pain, crouching over. ? Patient was thin and warm to touch. ? Bilateral wheezes. ? No other significant findings
- 6. ? Inferior anterolateral MI ? V4R showed involvement
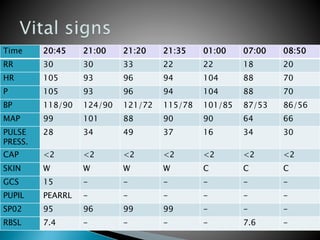
- 7. Time 20:45 21:00 21:20 21:35 01:00 07:00 08:50 RR 30 30 33 22 22 18 20 HR 105 93 96 94 104 88 70 P 105 93 96 94 104 88 70 BP 118/90 124/90 121/72 115/78 101/85 87/53 86/56 MAP 99 101 88 90 90 64 66 PULSE PRESS. 28 34 49 37 16 34 30 CAP <2 <2 <2 <2 <2 <2 <2 SKIN W W W W C C C GCS 15 - - - - - - PUPIL PEARRL - - - - - - SP02 95 96 99 99 - - - RBSL 7.4 - - - - 7.6 -
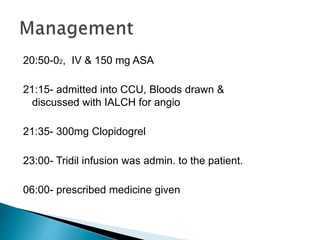
- 8. 20:50-02, IV & 150 mg ASA 21:15- admitted into CCU, Bloods drawn & discussed with IALCH for angio 21:35- 300mg Clopidogrel 23:00- Tridil infusion was admin. to the patient. 06:00- prescribed medicine given
- 9. ? Doctor°Øs prescription for patient management ? - Aspirin, 150mg daily PO (COX 1 & 2 Inhibitor) ? -Clopidogrel, 75mg daily PO (Anti-platelet- interferes with function) ? - Atorvastatin (Lipitor), 20mg daily PO (lowers LDL + Triglycerides) ? - Enalapril, 5mg daily PO (ACE-I) ? -Enoxaparin 60mg dly s/c (LMW Heparin)
- 11. ? EF of 42% ? LVA ? Thrombus formation in apex of LV
- 12. Persistent ST elevation shows Ventricular Aneurysm Ribeiro, A. L. et al. (2012) The infarcted muscle is replaced by a thin layer of collagenous scar tissue, that will gradually stretch as intraventricular pressure rises during systole.
- 14. ? Inferior anterolateral MI Follow up ? Patient discharged 25/07/13 ? Scheduled for angio on 25/09/13
- 15. The biggest problem for this patient was the inability of him and the family members to recognise that he was having a heart attack. This is one of the biggest delays to treatment and causes of a high mortality rate. If the patient had recognised that he was having an AMI all the resources would have been available. The patient would have had a better outcome and a better quality of life.
- 16. ? Physician, A.F. (2001) American Family Physician, 1 October, [Online], Available: http://www.aafp.org/afp/2001/1001/p1261.html [16 August 2013]. ? Early prevention of left ventricular dysfunction after myocardial infarction with angiotensin-converting- enzyme inhibition ? The Lancet, Volume 337, Issue 8746, Pages 872-876 N Sharpe, H Smith, J Murphy, S Greaves, H Hart, G Gamble ? Ribeiro, A. L. et al. (2012) Diagnosis and management of Chagas disease and cardiomyopathy Nat. Rev. Cardiol. doi:10.1038/nrcardio.2012.109