nasal polyp fix 2 koass haji tht 2016 pptx
ŌĆó
0 likesŌĆó10 views

nasal polyp fix 2 koass haji tht 2016 pptx


























nasal polyp fix 2 koass haji tht 2016 pptx
- 1. Nasal Polyp Consulent dr. Amran Simajuntak, Sp. THT-KL Author: Syahnita Mawarni LH Nuraini Syahputri Aulia Dini R
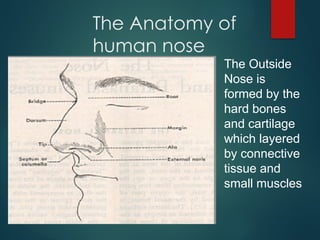
- 2. The Anatomy of human nose The Outside Nose is formed by the hard bones and cartilage which layered by connective tissue and small muscles
- 3. The Anatomy of human nose
- 4. The Anatomy of human nose
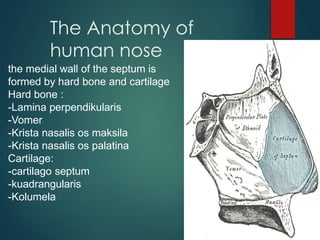
- 5. The Anatomy of human nose the medial wall of the septum is formed by hard bone and cartilage Hard bone : -Lamina perpendikularis -Vomer -Krista nasalis os maksila -Krista nasalis os palatina Cartilage: -cartilago septum -kuadrangularis -Kolumela
- 6. The Anatomy of human nose ’üĄThe Lateral wall is formed by : ’üĄ Konka ’üĄ Inferior ’üĄ Media ’üĄ Superior
- 8. The Anatomy of human nose Meatus - inferior : there is an estuary of nasolaclimary duct - media : estuary of frontal sinus, maxillary sinus, etmoid anterior sinus - Superior : estuary of etmoid posterior sinus and sfenoid sinus
- 9. The Anatomy of human nose The border of nasal cavity : -Inferior : formed by Os Maxilla and Os Palatum -Nasal Palate : formed by lamina kribiformis (part of Os Etmoid) - Posterior : formed by Os Sfenoid
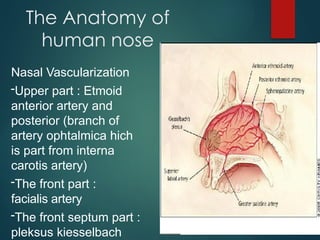
- 10. The Anatomy of human nose Nasal Vascularization -Upper part : Etmoid anterior artery and posterior (branch of artery ophtalmica hich is part from interna carotis artery) -The front part : facialis artery -The front septum part : pleksus kiesselbach
- 11. The Anatomy of human nose The nasal vein vascularization generally follow the arterial pattern. The vein have no vessel-valve
- 12. The Physiology of Human Nose ’üĄ Providing airway for respiration ’üĄ Moistening (humidifying) and warming the entering air ’üĄ Filtering inspired air and cleaning it of foreign matter ’üĄ Serving as a resonating chamber for speech ’üĄ Housing the olfactory reseptor
- 13. Nasal Polyps Benign mass that grow inside the nasal cavity Abnormal lesions that emanate from portion of nasal mucosa or paranasal sinuses Most polyp grow from etmoidal sinus mucose usually multiple or sometime billateral.
- 15. Nasal polyps ’üĄ Endoscopic view of left nasal cavity. Polyp protruding from uncinate process
- 16. Nasal polyps ’üĄ Left anterior nasal cavity showing an antro-coanal polyp. Sucker is pushing inferior turbinate to one side
- 17. Clasification
- 18. Pathophysiology ’üĄ Unknown ’üĄ Chronic inflammation ’üĄ Autonomic nervous system dysfunction ’üĄ Genetic predisposition ’üĄ Allergic verses non-allergic
- 19. Pathophysiology Associated with allergic conditions ’üĄ 20-50% have asthma ’üĄ Allergic rhinitis ’üĄ 8-26% have aspirin intolerance ’üĄ 50% have alcohol intolerance
- 20. Pathophysiology Non allergic conditions ’üĄ Cystic Fibrosis 6-48% have polyps ’üĄ AFS 85% have polyps ’üĄ Young syndrome ’üĄ Churg-Strauss syndrome
- 21. Pathophysiology ’üĄ Polyps are more common in patients with non-allergic asthma (13%) than allergic asthma (5%) ’üĄ 3000 atopic patients 0.5% have polyps Norlander et al (1999)
- 22. Pathophysiology Various theories ’üĄ Bernstein theory ’üĄ Vasomotor theory ’üĄ Epithelia rupture theory
- 23. Pathophysiology Bernstein theory ’üĄ Inflammatory changes in lateral nasal wall or sinus mucosa ’üĄ Polyps originate from contact area ’üĄ Ulceration, reepithelialisation and new gland formation ’üĄ Inflammatory processes from epithelial cells, endothelium and fibroblasts ’üĄ Integrity of sodium channels affected
- 24. Frequency ’üĄ Adults 1-4% ’üĄ Children 0.1% ’üĄ All races and social classes ’üĄ M/F 2-4:1 in adults ’üĄ Increasing incidence with age
- 25. Clinical Manifestation ’üĄ Asymptomatic ’üĄ Airway obstruction ’üĄ Postnasal drip ’üĄ Dull headaches ’üĄ Snoring ’üĄ Rhinorhoea ’üĄ Hyposmia / Anosmia ’üĄ Epistaxis (often other lesion) ’üĄ Obstructive sleep apnoea ’üĄ Craniofacial abnormalities ’üĄ Optic nerve compression
- 26. Differential ’üĄ Encephalocoeles ’üĄ Gliomas ’üĄ Dermoid tumours ’üĄ Haemangiomas ’üĄ Papillomas / transitional cell papillomas ’üĄ Nasopharyngeal angiofibromas ’üĄ Rhabdomyosarcomas ’üĄ Lymphomas ’üĄ Neuroblastomas ’üĄ Sarcomas ’üĄ Chordomas ’üĄ Nasopharyngeal carcinomas
- 27. Investigations ’üĄ Sweat test ’üĄ RAST / skin testing ’üĄ Nasal smear ’üĄ Microbiology ’üĄ Eosinophils (allergic component) ’üĄ Neutrophils (chronic sinusitis)
- 28. Investigations ’üĄ Coronal CT scan ’üĄ MRI scan ’üĄ Flexible nasendoscopy ’üĄ Rigid nasendoscopy
- 29. Treatment ’üĄ Oral and nasal steroids ’üĄ High dose prednisolone and nasal steroid for 20 days will eliminate 50% of polyps ’üĄ Lower bioavailability in modern nasal steroids ’üĄ Poor response in certain groups ’üĄ Intranasal injection not effective ’üĄ Immunotherapy ’üĄ Diet (no effect)
- 30. Treatment ’üĄ Traditional polypectomy ’üĄ Microdebrider ’üĄ Endoscopic sinus surgery ’üĄ Recurrence ’üĄ Multiple small polyps common ’üĄ Large and antro-coanal less so
- 31. Nasal polypectomy ’üĄ Nasal polyp. Stalk attached to medial maxillary wall
- 32. Nasal Polypectomy ’üĄ Microdebrider entering left middle meatus
- 33. Summary ’üĄ Common condition in adults ’üĄ Aetiology not fully understood ’üĄ Majority are not allergic in nature ’üĄ Medical treatment can be effective ’üĄ Even with surgery, recurrence is common
- 34. Any questions?