Necrotizing fasciitis
âĒDownload as PPTX, PDFâĒ
36 likesâĒ11,523 views

This was my short presentation on Necrotizing Fasciitis or as it is commonly known as "Flesh Eating Virus". Sorry if I am missing any point.

























Necrotizing fasciitis
- 1. SEGi College Sarawak FACULTY OF NURSING & ALLIED HEALTH Foundation in Science Necrotizing Fasciitis By Darrell Nadeng Dominic
- 2. âĒ Necrotizing Fasciitis is commonly known as âFlesh-eating diseaseâ or âFlesh-eating bacteria syndromeâ, is a RARE infection of the deeper layers of the skin and subcutaneous tissues. It can destroy muscles, skin and underlying tissue. âĒ âNecrotizingâ refers to something that causes body tissue to die.
- 3. What causes Necrotizing Fasciitis?
- 4. Necrotizing Fasciitis is commonly caused by Group A Streptococcus (GAS) bacteria, which is the same type of bacteria that causes strep throat. However, several types of bacteria, such as staphylococcus have also be associated with this disease.
- 5. An individual with Strep Throat
- 6. How do you obtain Necrotizing Fasciitis??
- 7. âĒ The bacteria that causes Necrotizing Fasciitis can enter the body following surgery or injury. They can also enter the body through : - Minor cuts - Insect Bites - Abrasions âĒ In some cases, it is unknown how the infection began. Once the infection takes place, it rapidly destroys muscles, skin and fat tissue.
- 8. The Symptoms
- 9. âĒ Increasing pain in the general area of a minor cut, abrasion, or other skin opening. âĒ Pain that is worse than would be expected from the appearance of the cut or abrasion. âĒ Redness and warmth around the wound, through symptoms can begin at other areas of the body. âĒ Flu-like symptoms such as diarrhea, nausea, fever, dizziness, weakness, an d general malaise. âĒ Intense thirst due to dehydration
- 10. More advance symptoms occur around the painful infection site within three or four days of infection. They include : âĒ Swelling, possibly accompanied by a purplish rash. âĒ Large, violet-colored marks that transform into blisters filled with dark, foul-smelling liquid. âĒ Discoloration, peeling, and flakiness as tissue death (gangrene) occurs.
- 11. Critical symptoms, which often occur within four to five days of infection, include : âĒ Severe drop in blood pressure âĒ Toxic shock âĒ Unconsciousness
- 12. Caucasian with necrotizing fasciitis. The left leg shows extensive redness and necrosis.
- 13. Diagnosis of Necrotizing Fasciitis
- 14. âĒ Diagnosis is often based on advance symptoms, such as the presence of gas bubbles under the skin. Laboratory analysis of fluid and tissue samples is done to identify the particular bacteria that are causing the infection. Treatment however, begins before the bacteria are identified. âĒ Household members and others who have had close contact with someone with necrotizing fasciitis should be evaluated if they develop symptoms of an infection.
- 15. Free air in the soft tissues due to necrotizing fasciitis
- 16. Necrotizing fasciitis causing air in soft tissues
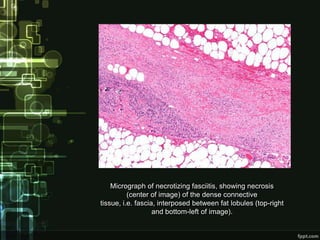
- 17. Micrograph of necrotizing fasciitis, showing necrosis (center of image) of the dense connective tissue, i.e. fascia, interposed between fat lobules (top-right and bottom-left of image).
- 18. Treatments for Necrotizing Fasciitis
- 19. Immediate treatment is needed to prevent death âĒ Powerful, broad-spectrum antibiotics given immediately through a vein (IV) âĒ Surgery to drain the sore and remove dead tissue âĒ Special medicines called donor immunoglobulin's (antibodies) to help fight the infection in some cases
- 20. Other treatments may include : âĒ Skin grafts after the infection goes away to help your skin heal and look better âĒ Amputation if the disease spreads through an arm or leg âĒ 100% oxygen at high pressure (hyperbaric oxygen therapy) for certain types of bacterial infections
- 21. Necrotic tissue from the left leg is being surgically debrided in a patient with necrotizing fasciitis
- 22. The left lower limb after extensive debridement
- 23. Prevention
- 24. âĒ Keep all wounds clean and watch closely for any signs of infection. Early detection and treatment of infection may be the best measure to prevent the subsequent development of necrotizing fasciitis. Promptly seek medical care if any signs or symptoms of infection appear.
- 25. âĒ Maintaining good personal hygiene and frequent hand washing can prevent infection and help control the spread of infection. Following guidelines of proper sterile surgical technique and practicing strict barrier (gloves, gowns, masks, etc.) and isolation precautions in hospitals can also allow health care personal prevent the development and spread of infection.
- 26. Aimee Copeland - aged 24 Survivor of Necrotizing Fasciitis
- 27. A 23 year-old woman developed a left facial cellulitis which progressed relentlessly with necrosis. Debridement was performed on several occasions to halt the spread of the necrosis. The ophthalmic team was consulted 10 days after her admission because of left ptosis. Examination revealed poor ocular movement, an urgent CT scan revealed cavernous sinus thrombosis. She was given anti-thrombotic treatment by the medical team. The facial defect was later reconstructed with myocutaneous graft from the thigh by the plastic team.
- 28. Conclusion?