










































































Pancreas Ca
- 2. CARCINOMA OF HEAD OF PANCREAS By DR. DANISH RAUF HOUSE OFFICER, CMH BAHAWALPUR Supervisor Col Malik Saeed Awan Assistant Professor and HOD Surgery Consultant General and Laparoscopic Surgeon CMH BWP
- 3. CMH BWP SEQUENCE â–ŞCase Presentation â–ŞCase Discussion
- 5. HISTORY PATIENT PROFILE • Name: XYZ • Age: 55 years • Gender: female • Residence: Bahawalpur • Date of presentation: 28 august , 2022 CMH BWP
- 6. PRESENTING COMPLAINTS Jaundice-01 year Itching- 01 day CMH BWP
- 7. HOPI JAUNDICE • My patient was in usual state of health 1 year back when she noticed yellowing of her eyes. CMH BWP
- 8. PRURITIS Patient also had complain of • Itching on whole body for last 2 months. • It was increasing progressively. • Relieved with medical ointment.
- 9. HOPI CONT • Had poor appetite • Loss of 1/3rd of body weight in last 2 months • Pale stools : last 1 year • Dark yellow urine There were no complaints of fever diarrhea or constipation
- 10. PAST HISTORY • Medical hx: DM Positive(7 Years) • Personal History: Poor Appetite Poor Bowel Habits • Drug History: Oral medications for diabetes • No hx of any drug or food allergies • Positive Family History CMH BWP
- 11. SYSTEMIC EXAMINATION • GPE: Well oriented in time place and person Jaundice positive • Vitals: BP: 130/90 mmHg Pulse: 92 bpm SPO2: 97% Temp: 98 degree F
- 12. SYSTEMIC EXAMINATION • Respiratory: • CVS: • CNS: • Musculoskeletal CMH BWP UNREMARKABLE
- 13. SYSTEMIC EXAMINATION • Abdominal Examination: • Inspection: unremarkable • Palpation: GB palpable 2 fingers below the right coastal margin No visceromegaly • Auscultation: BS normal
- 14. INVESTIGATIONS All baselines Blood CP: TLC:11.9 Hb : 9.1 Plt : 385 Clotting Profile: PT : 26 APTT: 48 Urine R/E: Colour : deep yellow CMH BWP
- 15. INVESTIGATIONS LFTS: •S.Total bilirubin : 245 (less than 17) •S. ALT : 103 (UPTO 36) •S. ALP : 1334 (LESS THAM 120) •S. AMYLASE : 183 HEP B and C Negative CMH BWP
- 16. RADIOLOGICAL FINDINGS • X-Ray: Normal study
- 17. • Ultrasound
- 18. CT SCAN
- 20. â–¶ Objectives: â–¶ anatomy â–¶ Epidemiology â–¶ Clinical features â–¶ Management
- 21. PANCREA S
- 25. NORMAL (50%)
- 26. CARCINOMA HEAD OF PANCREAS â–¶ Incidence is about 8 to 9 cases per 1,00,000 population. â–¶ 74% of patients die within the first year after diagnosis, with 5-year survival rate of only 6%.
- 28. RISK FACTORS – DEFINITIVE ASSOCIATION ▶Smoking 1 – 3 times risk, Directly proportional to the quantity and duration of smoking (i.e. pack year).
- 29. Obesity
- 30. DIET
- 32. LOCATION OF THE TUMOUR â–¶ About two-thirds of pancreatic adenocarcinomas arise within the head or uncinate process of the pancreas â–¶ 15% are in the body â–¶ 10% in the tail, â–¶ remaining tumours demonstrating diffuse involvement of the gland.
- 34. â–¶ TUMOURS IN THE HEAD OF THE PANCREAS ARE TYPICALLY DIAGNOSED EARLIER BECAUSE THEY CAUSE OBSTRUCTIVE JAUNDICE. â–¶ Tumours in the pancreatic body and tail are generally larger at the time of diagnosis, and therefore, less commonly resectable.
- 35. PRESENTATION - HISTORY â–¶ The classic constellation of symptoms in 66%- 75% of cases. â–¶ Painless, progressive Jaundice associated with â–¶ Pruritus â–¶ Acholic stools â–¶ High -coloured urine. â–¶ Pain,( left sided tumour present with pain) â–¶ cachexia
- 36. CLINICAL SIGNS
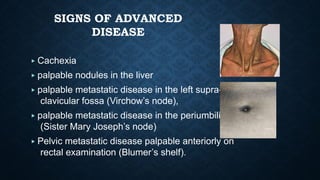
- 37. SIGNS OF ADVANCED DISEASE ▶ Cachexia ▶ palpable nodules in the liver ▶ palpable metastatic disease in the left supra- clavicular fossa (Virchow’s node), ▶ palpable metastatic disease in the periumbilical area (Sister Mary Joseph’s node) ▶ Pelvic metastatic disease palpable anteriorly on rectal examination (Blumer’s shelf).
- 38. VIRCHOWS NODE
- 39. SISTER MARY JOSEPH NODES Sister Mary Joseph’s node)
- 41. DR WILLIAM JAMES MAYO
- 42. BLUMMER SHELF
- 43. BIOCHEMICAL INVESTIGATIONS â–¶LFT â–¶ Elevated bilirubin, alkaline phosphatase and GGT â–¶ Only mild to moderate elevations in liver transaminases
- 44. CA 19-9 ▶ Used in cases where diagnosis is in doubt. ▶ Elevated in 75% of patients with pancreas cancer. ▶ also elevated in benign conditions of the pancreas, liver, and bile ducts. ▶ To measure response to therapy or for screening for recurrence ▶ Fallacy – can not be used in cases of jaundice.
- 45. IMAGING â–¶ ultrasonography â–¶ Computed tomography (CT), â–¶ Endoscopic ultrasound (EUS) â–¶ Magnetic resonance imaging (MRI) with or without magnetic resonance cholangio-pancreatography (MRCP) â–¶ Endoscopic retrograde cholangio-pancreatography (ERCP) â–¶ Positron emission Tomography (PET)
- 46. ULTRASONOGRAPHY
- 47. Dilated intrahepatic ducts. Double-duct sign” with dilated common bile duct and pancreatic ducts. CT SCAN
- 48. EUS
- 49. MRI images with gadolinium contrast.
- 50. MRCP of patient with obstructive jaundice.
- 51. ERCP â–¶ ERCP may be of benefit in patients with biliary obstruction and cholangitis - endoscopic stent can be placed for decompression. â–¶ With current capabilities of CT and MRI, ERCP is rarely necessary.
- 52. Endoscopic retrograde cholangiopancreatogram (ERCP) of patient with pancreas cancer with abrupt cut-off of main pancreatic duct secondary to tumor. ERCP of patient with pancreas cancer with obstruction of both main pancreatic duct and common bile duct
- 53. TISSUE DIAGNOSIS â–¶ A tissue diagnosis of adenocarcinoma is not required prior to an attempt at a curative resection. â–¶ â–¶ Does not change treatment decision in a planned curative surgery.
- 54. FNA IS REQUIRED IF 1. Patients undergoing neoadjuvant therapy. 2. If the diagnosis of carcinoma is uncertain.
- 55. STAGING â–¶ CT, EUS, MRI to detect local disease. â–¶ Chest x-ray with SOS CT chest, â–¶ Staging laparoscopy- varies between institutions.
- 56. AJCC STAGING
- 57. STAGE GROUPING
- 58. MANAGEMENT
- 60. ALLEN OLDFATHER WHIPPLE (1881-1963) ▶ Pancreatico-duodenectomy (PD) was first performed by Kausch in 1908, and popularized by Whipple in the 1930s (who performed 37 procedures). —Whipple AO, Parsons WB, Mullins CR. Treatment of Carcinoma of the Ampulla of Vater. Ann Surg 1935; 102: 763-769.
- 64. CHEMOTHERAPY â–¶ 5 FU alone or combination with radiotherapy â–¶ gemcitabine
- 65. PALLIATIVE TREATMENT â–¶ Relief of Jaundice
- 66. • Relief Of Duodenal Obstruction
- 67. Relief of pain 1 ) Morphine 2 ) Chemical Ablation of Celiac Ganglia
- 68. MCQS • The risk factors for pancreatic cancer includes all except: A. Diabetes mellitus B. Hereditary predisposition C. Chronic pancreatitis D. Smoking E . Acute pancreatitis
- 69. ANSWER E
- 70. The differential diagnosis of a mass lesion in pancreas includes all except: • The differential diagnosis of a mass lesion in pancreas includes all except: • 1. Lymphoma 2. Neuroendocrine tumour 3. Focal chronic pancreatitis 4. Autoimmune pancreatitis 5. None of the above
- 71. ANSWER E
- 72. • A 65 year old gentleman presented with dull aching upper abdominal pain radiating through to the back and worsened by eating. He had also noticed yellow discoloration of his skin and had lost weight. In his past medical history, he was diagnosed with diabetes mellitus 6 months earlier. A CT scan revealed a localised mass lesion in the head of pancreas with biliary duct dilatation. All the following are true except: • A. CT guided biopsy is needed to confirm the diagnosis B. A diagnosis of pancreatic cancer should be considered in unexplained diabetes (no family history, obesity or steroids) in patients over 50 years of age. C. Gastroduodenal artery encasement is not a contraindication for curative surgery D. Whipple’s operation is the standard operation for cancer of pancreatic head
- 73. ANSWER A