
















Pathology of Peptic Ulcer Disease
- 1. Presenter: AnilKr. Yadav PATHOLOGY OF PEPTIC ULCER ResourceFaculty: Dr. ParichaUpadhyaya Presenter:Anil Kr. Yadav
- 2. OBJECTIVES o Definition and pathogenesis of Peptic Ulcer o Morphology of Peptic Ulcer o Complications
- 3. DEFINITION Ulcer is defined as disruption of the mucosal integrity of stomach and/or duodenum leading to a local defect or excavation due to active inflammation. Erosion differs from an ulcer in being partial thickness mucosal defect. Peptic ulcers are chronic most often solitary lesions that occur in any portion of GIT exposed to the aggressive action of acid-peptic juices.
- 4. PROGRESSION
- 5. PATHOGENESIS Aggressive factors Defensive factors •Gastric acidity •Peptic enzymes •Surface mucus secretion •Bicarbonate secretion into mucus •Mucosal blood flow •Apical surface membrane transport •Epithelial regenerative capacity •Elaboration of PG
- 6. INJURY PEPTIC ULCER •H. Pylori infection •NSAID •Tobacco •Alcohol •Gastric hyperacidity •Duodenal-gastric reflux Impaired defenses •Ischemia •Shock •Delayed gastric emptying
- 8. RISK FACTORS FOR PUD •H. Pylori infection •NSAIDs •Cigarette use •COPD •Ilicit drugs like cocaine •Alcoholic cirrhosis •Psychological stress •Endocrine cell hyperplasia •ZE syndrome •Viral infection (CMV, HSV)
- 9. Organism attached to mucus-secreting cells of gastric mucosa by adhesins like BabA and SabA H. Pylori transmitted by fecal-oral/ oral-oral route In the stomach it swims in viscous mucus due to flagella Ammonia neutralizes HCl in stomach Production of large amount of ammonia from urea by bacterial urease Organism survival Inflammatory response Damage to mucus Gastritis and peptic ulcers
- 12. NSAIDS Membrane phospholipids Phospholipase A2 Arachidonic acid COX PG depletion Epithelial effects •Increase in HCl secretion •Decrease mucin secretion •Decrease HCO3- secretion •Decrease surface active phospholipids secretion •Decrease epithelial cell proliferation NSAIDs inhibits Endothelial effects Stasis ischemia
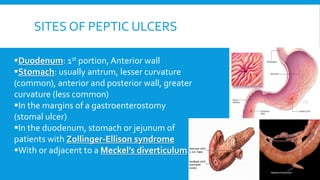
- 13. SITES OF PEPTIC ULCERS Duodenum: 1st portion, Anterior wall Stomach: usually antrum, lesser curvature (common), anterior and posterior wall, greater curvature (less common) In the margins of a gastroenterostomy (stomal ulcer) In the duodenum, stomach or jejunum of patients with Zollinger-Ellison syndrome With or adjacent to a Meckel’s diverticulum.
- 14. MORPHOLOGY GROSS •Round to oval, sharply punched-out defect •Mucosal margin usually level with the surrounding mucosa or only slightly elevated •Radiating mucosal folds •Base is smooth and clear, owing to the peptic digestion of exudates
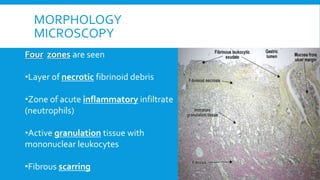
- 16. MORPHOLOGY MICROSCOPY Four zones are seen •Layer of necrotic fibrinoid debris •Zone of acute inflammatory infiltrate (neutrophils) •Active granulation tissue with mononuclear leukocytes •Fibrous scarring
- 17. CLINICAL FEATURES •Epigastric pain •Dyspepsia, including belching, bloating, distention, and fatty food intolerance •Heartburn •Chest discomfort •Hematemesis or melena resulting from gastrointestinal bleeding
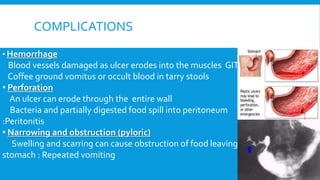
- 18. COMPLICATIONS • Hemorrhage Blood vessels damaged as ulcer erodes into the muscles GIT Coffee ground vomitus or occult blood in tarry stools • Perforation An ulcer can erode through the entire wall Bacteria and partially digested food spill into peritoneum :Peritonitis • Narrowing and obstruction (pyloric) Swelling and scarring can cause obstruction of food leaving stomach : Repeated vomiting
- 21. REFERENCES