


































phacodynamics basics what you need to know
- 1. PHACODYNAMICS Dr Osama Albarghouthi MD JBOphth FICO MRSCed
- 2. history The invention of phacoemulsification by Charles Kelman in 1967 marked the beginning of the modern era of cataract surgery. this advance also coincided with the invention of ophthalmic viscosurgical devices (ovds), the evolution of intraocular lens design, and a change to performance of cataract surgery on an outpatient basis, resulting in a paradigm shift that allowed cataract surgery to be performed via relatively small corneal incisions, leading to lower incidence of wound-related and vitreous-related complications and more rapid rehabilitation of vision. First surgery 3 hours + aphakic + rigid iol + 4 liter of fluid )))
- 3. Important factors for cataract surgery ŌĆó Biometry ŌĆó Surgical Skills + Technique + cataract ŌĆó Application Of Principles Of Phacodynamics
- 4. Instrumentation ’é× There are several types of phaco machines, but their major components are essentially the same. ’é× These include : ŌĆó Console ŌĆó The handpiece ŌĆó Foot pedal ŌĆó Irrigation system ŌĆó Pump
- 6. 0.05-0.1 mm (0,15,30,45,60) A tip with a steeper bevel has an oval port with a larger surface area, which can generate more holding force and greater cutting efficiency. The disadvantage of steeper bevels is that the larger opening may be more difficult to occlude to achieve full vacuum.
- 7. occlusion 1.Orientation 2.Impede deep 3.Listen to machine VRT
- 8. position 1 produces irrigation (no aspiration, no u/s). No linear control (on/off) position 2 irrigation and aspiration at a constant (panel) or variable (linear) rate (no u/s). position 3 irrigation, aspiration and u/s at a fixed (panel) or a variable (linear) rate.
- 10. The surgeon uses the handpiece to simultaneously emulsify and aspirate the crystalline lens while keeping the tip cool and maintaining anterior chamber depth without damaging posterior capsule or endothelium. FLUIDICS
- 11. Phaco power Phaco power is the percentage % of stroke length ŌĆó Amplitude ( how far ) to-and-fro oscillation which generate main forces for nucleus disassembly 1. Jack hammer effect longitudinal (grooving and chopping) & tortional (segment) 2. Acoustic shock wave & Cavitations ( microbubbles ) (more power % >> more impact >>more heat >> more damage to nucleus and the eye )) ŌĆó Frequency ( how often ) 40 KHZ fixed
- 13. Phaco Modes 1. Continuous: power is delivered constantly and is either linear or panel controlled (more ultrasound power- good for sculpting)
- 14. 2. Pulse mode: The term pulse describes an interval of phaco power turned on alternating with an interval during which phaco power is off (duty cycle concept). ŌĆóThe more the pedal is depressed, the higher the power in linear mode ŌĆóThe delivery of phaco power for only a portion of the cycle reduces repulsion ( chatter ) of material by the vibrating tip and improves followability ideal for quadrant removal
- 15. Duty cycle refers to the ratio of on:off pulses. If the time of ŌĆ£power onŌĆØ equals the time of ŌĆ£power off,ŌĆØ the duty cycle is 50%.
- 16. 3. Burst mode: Burst-mode phaco involves delivery of preset power (0%ŌĆō100%) in single bursts that are separated by decreasing intervals as the foot pedal is depressed through position 3. ŌĆó At the end of the position 3 excursion, the power is no longer delivered in bursts but is continuous. ŌĆó Burst mode allows the tip of the phaco needle to be buried into the lens, an essential step for chopping techniques.
- 17. Advanced phaco power mode delivery by J&J
- 18. Fluidics
- 19. Main concepts ŌĆó Maintain space (prevent collapse of AC by balancing inflow and outflow rates) ŌĆó Create currents (bring cataract pieces to phaco probe and remove them) ŌĆó Keep it cool (prevent thermal injury)
- 20. Fluidics parameters ŌĆó Mechanical ŌĆóInfusion/inflow/irrigation ŌĆóAspiration and leakage ŌĆóVacuum ŌĆó Clinical ŌĆóIncision size ŌĆóVitreous pressure
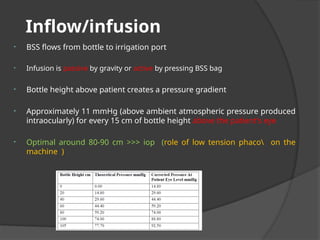
- 21. Inflow/infusion ŌĆó BSS flows from bottle to irrigation port ŌĆó Infusion is passive by gravity or active by pressing BSS bag ŌĆó Bottle height above patient creates a pressure gradient ŌĆó Approximately 11 mmHg (above ambient atmospheric pressure produced intraocularly) for every 15 cm of bottle height above the patient's eye ŌĆó Optimal around 80-90 cm >>> iop (role of low tension phaco on the machine )
- 22. Aspiration flow rate (AFR) ŌĆó Measured in ml/min ŌĆó Is determined by speed of pump ’é× As flow increases : current in AC increases: this determines how well particulate matter is attracted to the tip ŌĆó 15-20 trenching or sculpting 30-45 quadrant 25-30 chop & epinecleus 30-50 I&A 5-10 polish
- 23. Vacuum ŌĆó Create holding power ( negative pressure ) to keep material in phaco tip ŌĆó Created by a pump: ŌĆóPeristaltic pump: vacuum develops slowly ŌĆóVenturi pump: rapid rise in vacuum ŌĆó20-80 trenching or sculpting 400 quadrant 500 chop 300 epinecleus
- 24. AFR Vs Vacuum ŌĆó AFR is the rate at which fluid and emulsified nuclear particles are removed from the eye when the phaco tip is not occluded ŌĆó Vacuum is the negative pressure that builds up when the tip is occluded ŌĆó They are separate components that work hand in hand during outflow ŌĆó At low flow rates: gradual build up of vacuum (safe but slow) ŌĆó At high flow rates: faster vacuum build up (but less safe)
- 25. Pump ŌĆó Main function is to move fluid through the aspiration tubing ŌĆó Pump settings control rate of movement of fluid 1. Peristaltic pump (Flow based) ŌĆóAllows independent control of aspiration rate and vacuum level 2. Venturi pump (Vacuum based) ŌĆóAllows direct control of only vacuum level. Flow is dependent on vacuum level setting
- 27. ŌĆó Rollers move ŌĆó Compress the outflow tubing in a peristaltic manner ŌĆó ŌĆ£milkingŌĆØ action on fluid column ŌĆó The machine can control the flow level (flow based) ŌĆó A preset vacuum level is achieved once there is occlusion of outflow line (at low speed of rotation) ŌĆó By increasing the flow rate, vacuum is produced in the aspiration line without occlusion ŌĆó To build up vacuum without occlusion, you need to increase the flow rate (flow based pump)!!!! ’é×Active Control of Flow, Passive Change of Pressure
- 28. Venturi pump A Venturi pump creates a vacuum based on the Venturi principle: a flow of gas or fluid across a port creates a vacuum proportional to the rate of flow of the gas.
- 29. ŌĆó Vacuum is created within a rigid drainage cassette connected to the aspiration tubing ŌĆó No milking of the aspiration line’āĀ phaco tubing can be made rigid with low compliance ŌĆó Main advantage is the ability to create the preset vacuum level without occlusion of the phaco tip needle ŌĆó As the surgeon depresses the pedal, the preset vacuum is immediately created (vacuum based) ’é×Only the vacuum can be controlled. The flow rate is fixed and is a function of the vacuum ’é×Active Control of Pressure, Passive Change of Flow
- 31. Vacuum rise time ŌĆó The amount of time taken by the system to reach maximum vacuum setting once occlusion takes place ŌĆó Peristaltic pumps have a slower rise time (can be made faster by increasing the rotation of the wheel) ŌĆó Rise time ╬▒ AFR ╬▒ Pump Speed
- 32. AC stability ŌĆó Inflow=outflow at least but must be in>>out ŌĆó AC pressure has to be greater than vitreous pressure and atmospheric pressure (positive IOP) ŌĆó Under pressurization >>> collapse of AC’āĀ forward movement of iris and lens and posterior capsule ’āĀ rupture of posterior capsule ŌĆó One indicator of AC pressure imbalance is bouncing movement of iris and lens ŌĆó Over pressurization can lead to deepening of AC and zonular stress
- 33. Clinical Parameters ŌĆó Incision size: affects: ŌĆó Leakage ŌĆó Infusion ŌĆó Depends on external diameter of phaco tip ŌĆó Small incision causes infusion flow obstruction: squeezing of infusion sleeve’āĀ AC instability and build up of heat at the tip ŌĆó Big incision’āĀ more leakage ,AC instability and more astigmatism ŌĆó Vitreous pressure ŌĆó Patient dependent ŌĆó myopia hyperopia small orbit anesthesia speculum PXF aqueous misdirection LIRDS >>>>>>>Affects AC depth during phaco
- 34. Surge disbalance between in/out ŌĆóWhen the phaco tip is occluded ’āĀ negative pressure builds in the tubing ’āĀ collapse of the aspiration tube ’āĀ occlusion breaks after eating the nucleus piece ’āĀ tube returns to original shape ’āĀ surge (sudden sucking effect of fluid with AC shallowing (until infusion fluid compensates)).
- 35. How to reduce surge? ŌĆó Lower levels of flow and vacuum ŌĆó Increased bottle height ŌĆó Reduce leakage ŌĆó Aspiration bypass port (ABS) ŌĆó Venting ŌĆó Fusion ┬®┬«
- 36. Fusion ┬®┬« CASE Chamber Stabilization Environment
- 37. Deepest part of A/C DonŌĆÖt use 2nd instrument
- 38. Take home message ’é× Know your machine ’é× Know you skills ’é× Adopt your machine to your skills ’é× Accept the new technology ’é× Adopt your skills to new technology ’é× Pass knowledge & skills to juniors
Editor's Notes
- -fifth century bc.,COUCHING , was performed on mature cataracts. With the patient in a seated position, the surgeon inserted a needle or knife posterior to the corneoscleral junction and then pushed the lens inferiorly. -ICCE, was first performed in 1753 by Samuel Sharp. This procedure involved removing the lens with the capsule intact through a limbal incision by using a cryprobe. -17th century, Jacques Daviel (1696ŌĆō1762), extracted the cataract -rather than simply displacing it- by Creating an incision through the inferior cornea, enlarging the wound with scissors, incising the lens capsule, expressing the nucleus, and removing the cortex by curettage. -Albrecht von Graefe (1828ŌĆō1870) advanced this technique by developing a corneal knife ŌĆō CLEANER INCISION, BETTER HEALING.
- piezoelectric┬Āeffect, is the ability of certain materials (most commonly Quartz) to generate an AC (alternating current) voltage when subjected to mechanical stress or vibration, or to vibrate when subjected to an AC voltage, OR BOTH.
- Disatvanges are heat and chatter
- Followability: The ability of a fluidic system to attract and hold nuclear or cortical material onto the tip of an ultrasonic or irrigation/aspiration (I/A) handpiece until vacuum forces achieve evacuation.