

![Etiology:-
? The most frequent mechanism of injury is fracture.
? Other mechanisms of injuries to the physis include :-
?infection [Septic arthritis or metaphyseal osteomyelitis]
?tumor
?cysts
?vascular insult
?Repetitive stress injury [Gymnasts]
?Irradiation
?Neural involvement [in polio & Cerebral palsy]
?iatrogenic causes [surgical insults]
?Metabolic abnormalities [vit C def]](https://image.slidesharecdn.com/physialinjuries-230518055801-544c1243/85/Physial-Injuries-pptx-5-320.jpg)


















Physial Injuries.pptx
- 1. PHYSEAL INJURIES Presenter :- Dr. Danish Rauf l
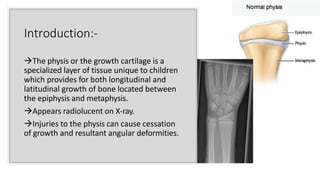
- 2. Introduction:- ?The physis or the growth cartilage is a specialized layer of tissue unique to children which provides for both longitudinal and latitudinal growth of bone located between the epiphysis and metaphysis. ?Appears radiolucent on X-ray. ?Injuries to the physis can cause cessation of growth and resultant angular deformities.
- 3. Prevalence ĻC 10 ĻC 30 % of all childhood fractures ? AGE :- INFANCY & 10-12 yrs of age. ? Males > Females ? Common sites :- Upper extremity > Lower Extremity -Phalanges are the most common site 37%, distal radius 18% and distal tibia 10%, other sites including distal femur ,proximal tibia/fibula.
- 4. Epiphyseal blood supply according to Dale & Harris ? TYPE A: Type A epiphyses are nearly completely covered by articular cartilage. Therefore, most of the blood supply to the epiphysis must enter from the perichondrium in a distal to proximal direction . This blood supply is susceptible to disruption by epiphyseal separation. The proximal femur and proximal humerus are examples of type A epiphyses. ? TYPE B: Type B epiphyses are only partially covered by articular cartilage. Such epiphyses are more resistant to blood supply impairment by epiphyseal separation. The distal femur, proximal and distal tibia, and distal radius are clinical examples of type B epiphyses.
- 5. Etiology:- ? The most frequent mechanism of injury is fracture. ? Other mechanisms of injuries to the physis include :- ?infection [Septic arthritis or metaphyseal osteomyelitis] ?tumor ?cysts ?vascular insult ?Repetitive stress injury [Gymnasts] ?Irradiation ?Neural involvement [in polio & Cerebral palsy] ?iatrogenic causes [surgical insults] ?Metabolic abnormalities [vit C def]
- 6. Clinical Presentation:- ? HISTORY :- - Pain / Swelling around the affected joint. - UPPER LIMB ? Function limited by pain. - LOWER LIMB ? Inability to bear weight. - History of trauma ? ON EXAMINATION :- - swelling + - Deformity +/- (minimal if present) - Focal tenderness over physis + - Limited ROM
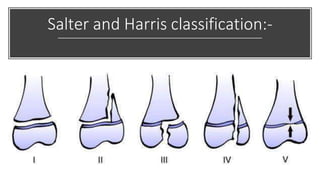
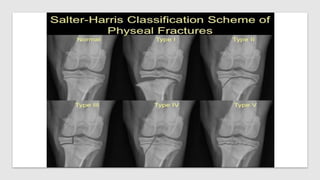
- 7. Salter and Harris classification:-
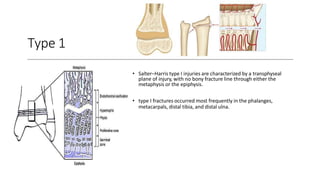
- 8. Type 1 ? SalterĻCHarris type I injuries are characterized by a transphyseal plane of injury, with no bony fracture line through either the metaphysis or the epiphysis. ? type I fractures occurred most frequently in the phalanges, metacarpals, distal tibia, and distal ulna.
- 10. Type 2 ? Type II injuries have physeal and metaphyseal components; the fracture line exits the physis to enter the metaphysis (i.e., away from the germinal and proliferative layers) at one margin. Similar to type I injuries, these fractures should have a limited propensity to growth disturbances.
- 12. Type 3 There are two fracture fragments: a small fragment consisting of a portion of the epiphysis and physis, and a large fragment consisting the remaining epiphysis and long bone. . higher risk of subsequent growth disturbance. ? Anatomic reduction (usually open reduction) and stabilization are required
- 14. Type 4 ? Type IV fractures are effectively vertical shear fractures, extending from the articular surface to the metaphysis. ? These fractures are important because ? they disrupt the articular surface, ? violate all the physeal layers in crossing from the epiphysis to the metaphysis ? may result in metaphysealĻCepiphyseal cross union which almost invariably results in subsequent growth disturbance. frequent around the medial malleolus ,lateral condyle of humerus.
- 16. ? In type 4, treatment principles include obtaining ? anatomic reduction ? adequate stabilization
- 17. Type 5 . ? Mechanism of this injury is by longitudinal compression, which damages the germinal layer of physeal cells. ? The prognosis for growth is poor, and there is a likelihood of premature growth cessation
- 19. General Principle of Treatment in Acute Physeal Injuries :- ? All reductions must be done with utmost gentleness to prevent further damage to the physis. Direct pressure on the physis by instruments must be avoided during open reduction. ? Microvascular disruption also plays a significant role to produce growth arrest.so,rather than trying multiple reductions ,more deformity after the # can be accepted, if the potential to remodel is high. ? Because of the intra-articular component, displaced type III and IV injuries must be reduced regardless of the time that has elapsed since the injury. ? Percutaneous pinning is often sufficient to stabilize the fragment. Cancellous cannulated screws of appropriate size may be used. Joystick method may be used to reduce the type III and IV fractures, to avoid open reduction (if possible).
- 20. ? Reduction:- ? The reduction maneuver must be performed as early as possible to prevent damage to the physis in the process of reduction. ? Each day of delay makes the reduction more difficult, especially in infants and younger child.
- 21. Methods of Reduction:- ? Type I and II: ? Injuries can be managed by closed reduction, as these cause less damage to the physis. ? Type III and IV: ? Might need open reduction to obtain anatomical reduction.
- 22. ? Caution must always be exercised during open reductions to prevent injury to the circulation entering the epiphysis. ? In Infants and newbornsĄŠany swelling near a joint, growth plate injury should be inspected unless otherwise proved by CT scans and MRI. ? The most desirable internal fixation is epiphysis to epiphysis and metaphysis to metaphysis if possible, especially in young children.
- 25. ? Period of immobilization and follow-up: ? Fracture is immobilized for at least 3ĻC4 weeks. ? No activities or play is allowed for at least 4ĻC6 weeks after removal of cast. ? Follow-up will be needed for at least 1 yr to 2 yrs after the treatment, and comparative radiographs of the contralateral limb should be taken
- 26. Complications of Physeal Injuries:- ?Growth Acceleration ?Malunion ?Nonunion ?Growth Arrest
- 27. ?Osteomyelitis ?Neurological Complications Median nerve compression in unreduced type II injury of distal radial epiphysis is known. ?Vascular Complications The popliteal artery is at risk in the physeal injuries around the knee following hyperextension injuries. Unrecognize damage or disruptions of the artery might lead to gangrene. ?Avascular Necrosis of Epiphysis Completely displaced type I physeal injuries of the femoral and radial head carry a high-risk of this complication. It results in cessation of growth.
- 28. THANK YOU