
















































POSTERIOR PALATAL SEAL. importance ,funtion,parts,anatomic and physiological
- 2. POSTERIOR PALATAL SEAL JANNU HARSHAVARDHAN I MDS 2
- 3. CONTENTS 3 ŌĆó DEFNITION ŌĆó INTRODUCTION ŌĆó IMPORTANCE OF POSTERIOR PALATAL SEAL ŌĆó PARTS OF POSTERIOR PALATAL SEAL ŌĆó FUNCTIONS OF POSTERIOR PALATAL SEAL ŌĆó ANATOMIC AND PHYSIOLOGIC CONSIDERATIONS OF PPS ŌĆó ANTERIOR AND POSTERIOR VIBRATING LINES ŌĆó CLASSIFICATION OF SOFT PALATE ŌĆó TYPES OF PPS ŌĆó TECHNIQUES OF RECORDING PPS ŌĆó TROUBLE SHOOTING ŌĆó RECENT ADVANCEMENTS ŌĆó CONCLUSION ŌĆó REFERENCES
- 4. 4 DEFINITION Posterior palatal seal: It is defined as ŌĆ£ the soft tissues along the junction of the hard and soft palates on which pressure within the physiologic limits of the tissues can be applied by a denture to aid in the retention of the denture.ŌĆØ ŌĆō GPT 9. E S S E N T I A L S O F C O M P L E T E D E N T U R E BY S H E L D O N W I N K L E R
- 5. INTRODUCTION 5 ŌĆó The proper placement of the posterior palatal seal begins with the initial oral examination. The morphologic contours of the hard and soft palate, hamular notch regions, as well as the integrity and displaceability of the mucosa and underlying glandular tissues, should be evaluated and noted. ŌĆó Hardy and Kapur stated that the retention and stability that is achieved from adhesion, cohesion, and interfacial surface tension are able to resist only those dislodging forces that act perpendicular to the denture base. ŌĆó The dislodgement of denture by lateral torque and horizontal forces could be resisted by retention provided by posterior palatal seal. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 6. 6 ’āś The peripheral seal of the maxillary denture is the area of contact the mucosa and the peripheral polished surfaces of the denture base; the seal prevents the passage of air between the denture and the tissues. This seal depends upon the proper extension of the denture borders, both in width and height, so that they fill the mucobuccal space and contact the cheek tissues laterally. ’āś At the posterior aspect of the denture, in the area of the soft palate, there are no cheek tissues to seal the denture border. Therefore; the proper placement of the posterior palatal seal commands a definite clinical procedural protocol if one is to create an optimally retentive complete maxillary prosthesis. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 7. IMPORTANCE OF POSTERIOR PALATAL SEAL 7 ’āś The addition of a proper border seal transforms into a very stable base that resists tipping thrust forces from all directions. ’āś Skinner has demonstrated the importance of the posterior palatal seal experimentally and stated that the most effective addition to increasing retention was the post dam. ’āś The posterior palatal seal will create a partial vacuum that will not operate continuously, it comes into play when horizontal or tipping thrusts tend to dislodge the denture then only to overcome the emergency. ’āś Posterior palatal seal complements the buccal and labial border seal converts the denture to a sealed compartment resisting torquing forces. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 8. FUNCTIONS OF THE POSTERIOR PALATAL SEAL AREA 8 1.It provides a close contact of the denture base with the mucous membrane which prevents food from getting under the denture. 2. It provides firm contact of the denture base with the tissue, and this diminishes or eliminates gagging. 3. It supplies sunken distal borders which are less conspicuous to the tongue. 4. It supplies a thick border to counteract denture warpage. 5. It adds confidence and comfort to patient by enhancing retention. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
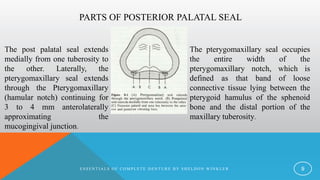
- 9. PARTS OF POSTERIOR PALATAL SEAL 9 The pterygomaxillary seal occupies the entire width of the pterygomaxillary notch, which is defined as that band of loose connective tissue lying between the pterygoid hamulus of the sphenoid bone and the distal portion of the maxillary tuberosity. The post palatal seal extends medially from one tuberosity to the other. Laterally, the pterygomaxillary seal extends through the Pterygomaxillary (hamular notch) continuing for 3 to 4 mm anterolaterally approximating the mucogingival junction. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 10. PTERYGOMAXILLARY NOTCH: ŌĆó The pterygomaxillary notch is covered by the pterygo mandibular fold, which extends from the posterior aspect of the tuberosity posterior-inferiorly to insert into the retromolar pad . This fold of tissue can influence the posterior border seal if the mouth is in a wide open position during the final impression procedure. ŌĆó It is important to note the exact position of the hamular process (located 2 to 4 mm posteromedial to the distal limit of residual ridge), since this will affect the length and direction of the pterygomaxillary seal. 10 ANATOMIC AND PHYSIOLOGIC CONSIDERATIONS OF PPS
- 11. 11 HAMULAR NOTCH ŌĆó The hamular process is covered by a thin layer of connective tissue One has to palpate the process in the course of outlining the posterior palatal seal area to realize the painful episode that the patient would experience if the denture base was extended to this area. ŌĆó Therefore hamular process should be never covered under denture. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 12. FOVEA PALATINI 12 ŌĆó There are two glandular openings within the tissues of the posterior portion of the hard palate, usually lying on either side of the midline. ŌĆó The fovea palatini, as they are known, are not constant findings in every individual; however, they are unique to humans. ŌĆó Therefore, the position of the fovea does not represent the junction of the hard and soft palates. The fovea palatini should be used only as guidelines to the placement of the posterior palatal seal E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 13. 13 ŌĆó The median palatal raphe, which overlies the medial palatal suture, contains little or no submucosa and will tolerate little compression. ŌĆó The judicious placement of the posterior palatal seal across the mid palatal suture in the region of the posterior nasal spine demands careful attention. ŌĆó When a prominent mid-palatal fissure is present on the hard palate, it often extends onto the soft palate. When the fissure is present, it should be carefully reproduced in the master cast. The posterior seal should be extended into this fissure to ensure proper peripheral seal. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 14. 14 ŌĆó The presence of thick, ropy saliva may create a problem for maxillary complete denture retention. Thick saliva can create hydrostatic pressure in the area anterior to the posterior palatal seal, resulting in a downward dislodging force exerted upon the denture base. ŌĆó A fine line or CupidŌĆÖs bow can be scribed on the master cast, anterior to the cluster of palatal mucous glands to alleviate this problem. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 15. ANTERIOR VIBRATING LINE 15 The anterior vibrating line is an imaginary line located at junction of the attached tissues overlying the hard palate and the movable tissues of the immediately adjacent soft palate. One way to locate the anterior vibrating is to have the patient perform the Valsalva maneuver, which requires that both nostrils be held firmly while the patient blows gently through the nose. This will position the soft palate inferiorly at its junction of hard palate. It can also be approximated by visualizing the area while instructing the patient to say ŌĆ£ ah " with short vigorous bursts. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 16. POSTERIOR VIBRATING LINE 16 The posterior vibrating line is An imaginary line at the junction of the aponeurosis of the tensor veli palatini muscle and the muscular portion of the soft palate. It represents the demarcation between that part of the soft palate that has limited or shallow movement during function (quivers) and the remainder of the soft palate that is markedly displaced during' functional movements. The posterior vibrating line is visualized by instructing the patient to say ŌĆ£ ah ŌĆØ in short bursts in a normal, unexaggerated fashion. It denotes the distal limit of denture. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 17. CLASSIFICATION OF SOFT PALATE 17 CLASS I: indicates a soft palate that is rather horizontal as it extends posteriorly, with minimal muscular activity. Class I palates are considered the most favorable configuration, since more retentive denture. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 18. 18 CLASS II: It indicates soft palate Class II designates those palatal contours that lie somewhere between class I and class III. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 19. 19 CLASS III: Class III indicates the most acute contour in relation to the hard palate, necessitating marked elevation of the musculature to create velopharyngeal closure. It is usually seen in conjunction with a high V -shaped palatal vault. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 20. DIFFERENT TYPES OF PPS 20 1) Bead type. 2) Double bead type. 3) Butterfly-type. 4) Butterfly type with bead on posterior limit. 5) Butterfly with widened with No. 9 round bur. 6) Posterior palatal seal constructed with reference to House classification, POSTERIOR PALATAL SEAL VARIATIONS BY ROGER AND JOHN YOUNG
- 21. TECHNIQUES OF RECORDING PPS 21 According to Hardy Kapur, there are 3 different types of recording PPS. ŌĆó FUNCTIONAL: In this method the final impression is moulded by the functional movement performed by the patient. ŌĆó SEMI FUNCTIONAL: Border moulding done by dentist. ŌĆó EMPIRICAL: Developed on cast by grooving the cast to desire depth. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 22. 22 The patient should be instructed to rinse with an astringent mouthwash to remove stringy saliva that might prevent clear transfer markings. CONVENTIONAL METHOD (Winkler method ) The posterior palatal area is then dried with gauze; a ŌĆ£T ŌĆØ burnisher or a mouth Mirror is used to palpate for the hamular processes. Once located, they should be marked with an indelible pencil or noted visually to ensure that they are not covered by denture. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 23. 23 The instrument (ŌĆ£T ŌĆØ burnisher or mouth mirror) is then placed along the posterior angle of the tuberosity until it drops into the pterygo maxillary notch. Through the notch and extended 3 to 4 mm anterolateral to the tuberosity, approximating the mucogingival junction. The same procedure is then performed on the opposite side. The patient is asked to say ŌĆ£ ah ŌĆØ in short bursts in an unexaggerated fashion. the posterior vibrating line is marked with an indelible pencil. By connecting the line through the pterygomaxillary seal with the line just drawn demarcating the posterior vibrating line, the posterior denture extension is delineated. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 24. 24 The resin or shellac tray is then inserted into the mouth and seated firmly to place. Upon removal from the mouth, the indelible lines should have been transferred to the tray, which in turn transfer to cast to complete the transfer of the posterior border is trimmed. ŌĆ£T ŌĆØ burnisher or mouth mirror determines their compressibility in width and depth. The termination of the glandular usually coincides with the anterior vibrating line. The use of the Valsalva maneuver .ŌĆÖ or the area while the patient saysŌĆÖ ah" vigorous bursts may also be marked with an indelible pencil and transferred to the master cast. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 25. 25 A Kingsley scraper is then used to score the cast. The deepest areas of the seal are located on either side of the midline, one-third the distance anteriorly from the posterior vibrating line. It is usually scraped to a depth of approximately 1 to 1.5 mm As the seal approaches the anterior vibrating line there is just a slight scraping of the cast. Just posterior to the deepest portion of the seal, it is also tapered to the posterior vibrating line. Failure to taper the seal posteriorly may lead to tissue irritation. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 26. 26 Shellac base can be re-adapted to reconfirm the scored cast is verified in the patientŌĆÖs mouth for the retentive property. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 27. ADVANTAGES 27 1. The trial base will be more retentive; this can produce more accurate maxilla mandibular records. 2. Patients will be able to experience the retentive qualities of the trial base, giving them the psychological security of knowing that retention will not be a problem in the completed prosthesis. 3. The practitioner will be able to determine the retentive qualities of the finished denture, leaving nothing to chance at the insertion appointment. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 28. DISADVANTAGES 28 1. It is not a physiologic technique and therefore depends upon accurate transfer of the vibrating lines and careful scraping of the cast. 2. The potential for over-compression of the tissues is great. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 29. 29 FLUID WAX TECHNIQUE 1. In this method the indelible transfer markings are recorded on the final wash impression. Zinc oxide and eugenol or plaster are preferred over the elastic impression materials, as they are set rigid. 2. Impressions made with elastic materials are slightly resilient, and when reseated in the mouth under pressure may distort the relationship between wax added to the posterior border and the rest of the denture-bearing surface. 3. All procedures of location and transferring the anterior and posterior vibrating line are same as conventional approach. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 30. 30 Materials used in fluid wax technique Zinc oxide eugenol impression is preferred over elastic impression material. The different types of waxes used are 1. Iowa Wax (White) - Dr. Earl S.Smith. 2. Korecta Wax no 4 (Orange) - Dr.O.C.Applegate. 3. H L physiological paste (Yellow ŌĆō White) - Dr. C.S Howkins. 4. Adaptol (Green) - Dr.Nathan. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 31. 31 1. Any of four mouth temperature waxes is used to paint on the impression surface of the posterior seal area and allowed to cool below room temperature to increase itŌĆÖs consistency and make it more resistant to flow. 2. While maintaining the 30┬░ flexion of the head and the anterior tongue position, the patient is asked to periodically rotate the head so that all functional positions of the soft palate are recorded. 3. After 4-6 minutes, the impression tray is removed from the mouth and wax examined for through contact. 4. Where tissue contact doesnŌĆÖt contact it appears as dull and if tissue has been contacted it appears as glossy surface. FLUID WAX TECHNIQUE E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 32. 32 5. The secondary impression is reinserted and held for three to five minutes under gentle pressure, followed by two to three minutes of firm pressure applied to the mid-palatal area of the impression tray. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 33. 33 ADVANTAGES 1. Physiological displacing of tissues occurs within physiologically acceptable limits. 2. Over compression of tissues is avoided. 3. Mechanically scraping of cast is not required. DISADVANTAGES 1. More time-consuming method. 2. Difficulty in handling material. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 34. SEMI FUNCTIONAL METHOD 34 ŌĆó In this method, the dentist performs the border moulding. ŌĆó Border moulding determines the extension by functional and manual manipulation of tissues. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 35. ARBITRARY SCRAPING OF MASTER CAST 35 1. Anterior and posterior vibrating line are visualized by examining the patientŌĆÖs mouth and are approximately marked on the master cast. 2. The least accurate leaves the chance of tissue compressibility. 3. Inaccurate and not physiological. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 36. 36 BOUCHER TECHNIQUE The width of the posterior palatal seal is limited to bead on denture with 1.5 mm depth and 1.5 mm height. YA B IN D H O O E T A L P O S T E R IO R PA LATA L S E A L A LIT E R AT U R E R E V IE W
- 37. BERNARD LEVIN METHOD IN CLASS III 37 YA B IN D H O O E T A L P O S T E R IO R PA LATA L S E A L A LIT E R AT U R E R E V IE W
- 38. BERNARD LEVINS METHOD IN CLASS I AND II PALATE 38 YA B IN D H O O E T A L P O S T E R IO R PA LATA L S E A L A LIT E R AT U R E R E V IE W
- 39. SWENSONŌĆÖS METHOD 39 YA B IN D H O O E T A L P O S T E R IO R PA LATA L S E A L A LIT E R AT U R E R E V IE W
- 40. SWENSONŌĆÖS TECHNIQUE 40 YA BINDHOO ET AL POSTERIOR PALATAL SEAL A LITERATURE REVIEW
- 41. ADDING PPS TO EXISTING DENTURE 41 There are numerous techniques to improve the posterior palatal seal on an existing denture. Moghadam and Scandrett suggest a procedure that utilizes the fluid wax technique. All of the steps outlined for locating, marking, and placing the wax in the seal area are followed, except that this time the wax is placed on the processed denture base. After the wax has had an adequate chance to flow, the denture is re moved from the mouth. An indelible pencil is used to outline the anterior extent of the seal on the denture. Utility wax is placed vertically across the palate, separating the posterior two-thirds from the anterior region, and extended around the posterior portion of the denture. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 42. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R 42 After PPS is recorded, the denture is removed from the mouth. The stone is vibrated on the denture wax surface After the stone is set wax is eliminated. The auto-polymerizing acrylic powder is sprinkled between the denture base and cast while holding on vibrator. The monomer is added drop wise the denture is relaced on stone cast and held with rubber bands. Then they are placed in the pressure pot with water 140 F for 20 minutes under 30 psi pressure. After the denture and cast are separated ,the excess acrylic is trimmed and border is polished lightly .
- 43. TROUBLESHOOTING OF PPS 43 Overextension: The most common complaint of patient where swallowing is painful and difficult. Small ulcers are seen in the region of the soft palate. If the hamuli are covered in denture the patient feel pain during the function and experience pain. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 44. OVER POST DAMMING 44 Over-scrapping of the master cast produces the posterior palatal seal displaces to much tissue compressibility is seen. Significant over-post damming causes the posterior border displaces inferiorly. Moderately over post-damming causes tissue irritation across the posterior palatal region. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 45. UNDER EXTENSION 45 Commonly, this is a result of the practitionerŌĆÖs use of the fovea palatini as the landmark for terminating the denture base. By so doing, he may be depriving the patient of as much as 4 to 12 mm of tissue coverage, which can significantly improve the retentive qualities of the denture. Over-trimming of the denture by the lab technician. Due to fear over gaging the dentist tries to over-trim the denture. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 46. UNDER POST DAMMING 46 When the mouth is in the wide open position, the pterygomandibular fold becomes taut. When the patient assumes any position other than a wide open position, a space will be present between the denture base and the tissue, since the fold is no longer activated. The diagnosis of this condition consists of placing the wet denture base into the mouth and slowly pressing in the midpalate region until it is firmly seated, all the while observing the distal denture border. If air bubbles can be seen escaping from beneath the distal border. E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 47. 47 YA B IN D H O O E T A L P O S T E R IO R PA LATA L S E A L A LIT E R AT U R E R E V IE W
- 48. RECENT ADVANCEMENTS 48 The use of an intraoral scanner may help in recording completely edentulous jaws, particularly in patients with flabby ridges or with undercuts, where conventional impression-making may be challenging. Digital intraoral scans are also useful when fabricating immediate complete dentures, in particular, when teeth are mobile or in a position making conventional impressions difficult. Nevertheless, digital scans have drawbacks, as they can produce a mucostatic recording of the tissues but fail to capture the appropriate extension of the movable tissues.
- 49. 49 The molding of a peripheral border in function is still not possible with a digital intraoral scan and the standard impression for CD fabrication consists of molding the peripheral border with a plastic material and subsequently loading the custom tray with a zinc oxide/ eugenol-based paste or an elastomer. A combination of conventional border molding and an intraoral scan has been described to compensate for the shortcomings of the scan. A definitive cast was made by combining the digital files from the scan and those issued from a border- molded custom tray. However, this interesting technique requires an additional software program operation to combine the information from the 2 recording Najila et al Fit and retention of complete denture bases: Part II e conventional impressions versus digital scans: A clinical controlled crossover study .JPD
- 50. CONCLUSION 50 1. Placement of the correct posterior palatal seal is given importance in complete denture fabrication. 2. Following established techniques for placement of border seal will ensure the retentive prosthesis 3. Careful examination during the diagnostic phase of the treatment can alleviate many potential problems . E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 51. REFERENCES 51 1. Essentials of the complete denture by Sheldon Winkler. 2. Prosthodontic treatment for edentulous patients by Zarb Bolender. 3. Hardy IR, posterior border itŌĆÖs Rationale and Importance J Prostheth Dent. 4. Winland, Young Maxillary complete denture posterior palatal seal, variations in size, shape, and location. 5. YA Bindhoo et al Posterior palatal seal a Literature review . E S S E N T IA LS O F C O M P LE T E D E N T U R E B Y S H E LD O N W IN K LE R
- 52. 52
Editor's Notes
- #12: O re