Powerpoint
Download as ppt, pdf0 likes1,754 views

This document discusses growth assessment and growth disorders. It begins by providing questions to ask parents to assess possible growth issues. It then discusses evaluating suspected growth abnormalities, including considering pregnancy/birth history, general health history, growth charts, and family history. The document provides guidance on monitoring growth accurately over time. It also outlines the diagnostic workup and potential causes of short stature, including endocrine and non-endocrine systemic disorders. The history and current use of growth hormone therapy is reviewed.
1 of 73
Downloaded 21 times

![Growth and Growth Disorders
Diagnostic Workup
Initial Screening Tests
’üČ Complete blood cell count (CBC)
’üČ Erythrocyte sedimentation rate (ESR)
’üČ Blood chemistries, including electrolytes
’üČThyroid profile (L-thyroxine [T4] and thyrotropin
[TSH])
’üČ Kidney profile (urinalysis [UA], blood urea nitrogen
[BUN], creatinine)
’üČ Bone age (BA)](https://image.slidesharecdn.com/powerpoint-140304115351-phpapp01/85/Powerpoint-13-320.jpg)
Recommended
Disorder of adernal gland
Disorder of adernal glandDR .PALLAVI PATHANIA
╠²
The adrenal glands are located above the kidneys and produce several important hormones. The adrenal cortex produces cortisol, aldosterone, and androgens. Cortisol aids metabolism and reduces inflammation. Aldosterone regulates sodium and potassium levels. Androgens influence sex drive. The adrenal medulla produces epinephrine and norepinephrine which help the body respond to stress. Diseases can occur if the adrenal glands produce too much or too little of these hormones.Pubertal disorders
Pubertal disordersDr. Nitish kumar
╠²
Disorders of pubertal development can involve delayed, premature, or arrested puberty. The document discusses the normal physiology of puberty and various conditions that cause abnormalities in pubertal development, including central precocious puberty, peripheral precocious puberty, premature adrenarche, constitutional delay of growth and puberty, and pubertal arrest. Evaluation and management of disorders of pubertal development involves assessment of signs of puberty, auxiliary investigations, and potential treatments depending on the underlying cause.Puberty
PubertyRyan Paul Floralde
╠²
This document discusses puberty and precocious puberty in females. It defines puberty as the physiological phase of development lasting 2 to 5 years where the genital organs mature. Signs of puberty in females include menarche, development of secondary sex characteristics, physical development, and psychological changes. Precocious puberty is defined as the appearance of any secondary sex characteristics before age 8. The document discusses the types, causes, diagnosis, and treatment of precocious puberty. The treatment aims to arrest maturation until the normal age while maximizing adult height.hyperprolactinemia
hyperprolactinemiaSreelasya Kakarla
╠²
This document discusses prolactinomas, which are pituitary tumors that cause excessive prolactin secretion. It describes the clinical presentation, diagnosis, and management approaches for prolactinomas. Microprolactinomas are small tumors less than 10mm, while macroprolactinomas are larger tumors. The first line treatment is dopamine agonist medication to reduce prolactin levels. Surgical removal may be considered for resistant cases or tumors pressing on nearby structures. Prolactinomas are generally managed medically but require monitoring due to risks of vision changes or hypogonadism from high prolactin levels.Normal puberty
Normal pubertyraj kumar
╠²
The document discusses the normal physiological process of puberty in humans. It describes the prepubertal period and the three changes that occur: adrenarche, decreasing repression of the hypothalamic-pituitary system, and gradual amplification of the interaction between GnRH and gonadotropins. It also discusses the stages of pubertal development, timing of puberty which is influenced mostly by genetics, and average ages for the different Tanner stages of breast and pubic hair development.Male hypogonadism
Male hypogonadismibrahimkiwan1
╠²
Male hypogonadism is a condition where the body does not produce enough of the male sex hormone testosterone. There are two types: primary, where the problem originates in the testicles, and secondary, where it is caused by issues with the hypothalamus or pituitary gland in the brain. Untreated hypogonadism can lead to complications like abnormal genitalia, infertility, erectile dysfunction, and osteoporosis. Diagnosis involves hormone testing, semen analysis, and imaging, while treatment is testosterone replacement therapy.Adrenal gland disorders kinara
Adrenal gland disorders kinaraKinara Kenyoru
╠²
This document discusses adrenal gland disorders. It describes the anatomy and functions of the adrenal cortex and medulla. It then covers various adrenal disorders including adrenal hypofunction (such as Addison's disease), hyperfunction (Cushing's syndrome and hyperaldosteronism), congenital adrenal hyperplasia, and adrenal crisis. It provides details on the causes, clinical presentations, investigations, and management of these various adrenal disorders.Delayed Puberty Topics in Adolescent Gynecology Delayed Puberty Topics in A...
Delayed Puberty Topics in Adolescent Gynecology Delayed Puberty Topics in A...MedicineAndHealth14
╠²
This document discusses delayed puberty in adolescent girls. It begins by outlining normal pubertal development and defining delayed puberty. Delayed puberty is then classified into three categories: hypergonadotropic hypogonadism (43%), hypogonadotropic hypogonadism (31%), and eugonadism (26%). For evaluation and management, the document recommends obtaining a history, physical exam, initial labs (TSH, prolactin), and a progestational challenge to determine gonadotropin levels and identify underlying causes. Treatment strategies aim to correct the underlying pathology, prevent disease complications, and provide sex steroids.Cushing syndrome
Cushing syndromeAnitha Dsouza
╠²
Cushing's disease is a hormonal disorder characterized by prolonged exposure to elevated cortisol levels, often caused by benign tumors or excessive use of cortisone medication. Symptoms include obesity, rounded face, muscle wasting, and increased susceptibility to infections, among others. Diagnosis involves various tests, and treatment may include surgery, medications to suppress cortisol production, and management of associated health issues.Puberty normal and precocious
Puberty normal and precociousAbdulmoein AlAgha
╠²
Additional important history:
- Family history of precocious or early puberty
- Developmental milestones
- Medications/supplements
Examination:
- Bone age X-ray
- Pelvic/abdominal ultrasound
- MRI brain
Differential diagnosis:
- Central precocious puberty
- Peripheral precocious puberty (e.g. McCune-Albright syndrome)
- Pseudoprecocious puberty
Investigations:
- LH, FSH, estradiol
- Chromosome analysis
- MRI to rule out CNS pathology
Final diagnosis: Central precocious puberty likely due to early activation of hypDelayed puberty ppt
Delayed puberty pptYassin Alsaleh
╠²
This document provides information on evaluating and treating delayed puberty. It defines delayed puberty and discusses the main causes, which include constitutional delay of puberty, hypogonadotropic hypogonadism, and hypergonadotropic hypogonadism. Evaluation involves assessing medical history, physical exam including Tanner staging, lab tests of hormone levels, bone age, and imaging if needed. Treatment depends on the underlying cause, and may include observation, sex hormone therapy, or treating any underlying medical conditions.Male Hypogonadism
Male HypogonadismSiti Nurul Afiqah Johari
╠²
Male hypogonadism is caused by androgen deficiency which can negatively impact organ functions and quality of life. The goal of testosterone replacement therapy is to restore hormone levels to the normal range and alleviate symptoms. Common treatment options include injections, patches, gels, and implants which can restore sexual function, muscle strength, and bone density. Therapy requires monitoring for side effects like prostate issues or blood clots. Gonadotropins may also be used to stimulate testosterone production and spermatogenesis in hypogonadotropic hypogonadism.Disorder Of Puberty
Disorder Of Pubertydavinpratama
╠²
1) Puberty is the biological changes and sexual maturation that occur during the transition from childhood to adulthood, with the average age of onset being 10-13 years for girls and 12-15 years for boys.
2) Precocious and delayed puberty are disorders defined by puberty onset more than 2 standard deviations outside typical ages. Evaluation of puberty issues includes medical history, physical exam focusing on growth and sexual development, and basic lab tests.
3) Common causes of delayed puberty include constitutional delay, chronic illnesses, nutritional deficiencies, and hormonal disorders; while precocious puberty can be gonadotropin-dependent or -independent. Health care providers must provide long-termPuberty
PubertyAbdulmagid Sarhan
╠²
1) Puberty is the process of physical maturation from child to adult, triggered by hormonal changes. It involves growth, development of secondary sex characteristics, and reproductive ability.
2) The timing of puberty is influenced by genetics as well as environmental factors like nutrition and geography. It typically occurs between ages 8-13 in girls and 9-14 in boys.
3) Precocious puberty describes the onset of puberty before age 8 in girls and age 9 in boys. It can be caused by genetic conditions, brain abnormalities, or tumors and requires medical evaluation and sometimes treatment to delay puberty.Female sex hormones
Female sex hormonesShipra Jain
╠²
This document provides information about estrogens including their biosynthesis, mechanisms of action, pharmacological actions, therapeutic uses, and adverse effects. It discusses natural and synthetic estrogens as well as selective estrogen receptor modulators. Key points include that estradiol is mainly produced in the ovaries and adrenals and acts by binding to nuclear estrogen receptors. Estrogens have various effects in the female reproductive system as well as secondary sex characteristics, bone, brain, liver, and cardiovascular system. Therapeutic uses include hormone replacement therapy and contraception, while adverse effects include an increased risk of certain cancers.Thyroid Hormone
Thyroid HormoneAbdul Wahab
╠²
The document discusses the anatomy, production, regulation, actions, and disorders of the thyroid gland and thyroid hormones. It describes how thyroid hormones are produced in the thyroid gland, transported through the blood, and regulate metabolism and growth through feedback mechanisms involving the hypothalamus and pituitary gland. The summary also discusses hyperthyroidism and hypothyroidism, which can result from excess or deficiency of thyroid hormones.A young boy with signs of puberty
A young boy with signs of pubertyMashfiqul Hasan
╠²
This case discusses a 7-year-old boy presenting with early signs of puberty over the past 5-6 months. Laboratory tests showed elevated levels of testosterone, LH, and FSH, confirming precocious puberty. A GnRH stimulation test showed an LH spike, indicating central precocious puberty. The patient was diagnosed with idiopathic central precocious puberty and prescribed injections of Decapeptyl to delay further pubertal progression until age 11 in order to avoid short adult stature. The document discusses evaluation and management of precocious puberty.Pediatric dosage calculation tutorial 2011(1).ppt
Pediatric dosage calculation tutorial 2011(1).pptJames_Pearce
╠²
This document provides guidance on pediatric dosage calculation, which differs from adult dosage calculation in that doses are based on body weight in kilograms and recommended ranges rather than standard doses. It covers converting weight from pounds to kilograms, writing medication orders, calculating liquid medication doses, reading medication labels, rounding rules, and intravenous drip rates. Practice problems are provided to help learn these concepts.Addison disease
Addison diseaseGagan Velayudhan
╠²
Addison disease is caused by primary adrenocortical deficiency due to destruction of the adrenal cortex, most commonly from autoimmune disease or tuberculosis. It presents with weakness, weight loss, hyperpigmentation, and hypotension due to glucocorticoid and mineralocorticoid deficiency. The diagnosis is made by demonstrating a subnormal response on ACTH stimulation testing with failure to increase cortisol levels above the normal range.Delayed puberty in children
Delayed puberty in childrenAbdulmoein AlAgha
╠²
This document discusses delayed puberty in children. It begins by defining normal puberty and factors that can affect the timing of puberty. It then defines delayed puberty and describes the main types as hypogonadotropic hypogonadism, characterized by low gonadotropins, and hypergonadotropic hypogonadism, characterized by high gonadotropins. The document outlines the evaluation and management of delayed puberty, including history, physical exam, laboratory tests, and treatment approaches depending on the underlying cause. Treatment may involve hormone replacement therapy, addressing underlying medical conditions, or observation in cases of constitutional delay.Puberty dr-arshiyasultana-110312042731-phpapp02
Puberty dr-arshiyasultana-110312042731-phpapp02Asri Purwanti
╠²
Puberty is the transition period between childhood and adulthood that involves physical and hormonal changes. Precocious puberty refers to the onset of puberty before age 8 in girls and age 9 in boys. It can be classified as central, peripheral, or combined based on whether the cause is in the brain or peripheral organs. Diagnosis involves physical exams, hormone tests, imaging, and puberty staging. Treatment depends on the type but may include medication to delay puberty or surgery to remove tumors.Disorders of puberty.pptx 2
Disorders of puberty.pptx 2Whiteraven68
╠²
The document discusses various topics related to puberty, including definitions of key terms, the normal sequence and timing of pubertal changes, causes and treatment of precocious and delayed puberty, and case studies. Precocious puberty can be true/idiopathic, due to tumors or other medical issues, or pseudopuberty caused by medication or conditions like premature adrenarche. Delayed puberty may be due to constitutional delay, medical issues impairing the HPA axis, or prior treatments like radiation therapy. Evaluation and management depends on the underlying cause and aim to initiate puberty normally or replace missing hormones.Normal puberty
Normal pubertyWhiteraven68
╠²
Puberty is the stage of physical maturation triggered by increased secretion of hormones like Luteinizing Hormone and GnRH, resulting in sexual and somatic development. It involves breast development in females starting around age 10-14 and testicular growth in males around age 12-16. Puberty encompasses five stages of physical changes through Tanner stages including growth spurts that make individuals reproductively mature.Addison's Disease
Addison's DiseaseHector Chavez
╠²
Addison's disease is a rare endocrine disorder where the adrenal glands do not produce enough hormones. It is caused by damage to the adrenal cortex, which can be from an autoimmune response, infection, tumors, or other issues. Symptoms include weakness, fatigue, weight changes, and hyperpigmentation of skin. Left untreated, it can cause an Addisonian crisis with severe low blood pressure and other dangerous symptoms. Treatment involves lifelong hormone replacement therapy and monitoring, especially during times of stress. Nursing care focuses on monitoring the patient, educating on treatment and crisis signs, and ensuring fluid and electrolyte balance.Thyroid disorder's
Thyroid disorder'sShubhamSonwane2
╠²
Thyroid disorders can cause the thyroid gland to function abnormally. The document discusses several thyroid disorders including hyperthyroidism (overactive thyroid), hypothyroidism (underactive thyroid), Graves' disease, goiter and thyroiditis (inflammation of the thyroid). It provides details on the causes, symptoms, diagnosis and treatment of these conditions. Thyroid function tests are used to evaluate thyroid function and monitor treatment for thyroid disorders.Precocious puberty
Precocious pubertyKelvin Philip
╠²
1) Precocious puberty is the onset of secondary sexual characteristics before age 8 in girls and age 9 in boys. It can be caused by premature activation of the hypothalamic-pituitary-gonadal axis (central) or premature sex hormone secretion from other sources like the adrenal glands (peripheral).
2) Treatment involves suppressing sex hormone production using GnRH analogues to stop further sexual development and rapid growth. This helps preserve final adult height.
3) Pubertal development is assessed using the Tanner stages, which evaluate breast/genital development and pubic hair growth. Precocious puberty disrupts the normal timing and progression of these stages.Endocrinology thyroid disorder
Endocrinology thyroid disorderLih Yin Chong
╠²
A 27-year-old female presents with palpitations. Exam finds an enlarged, tender thyroid. Labs show suppressed TSH, elevated T4 and low radioactive iodine uptake. The next appropriate test would be to check the ESR, as these findings are consistent with subacute thyroiditis, an inflammation of the thyroid gland often caused by a viral infection. The treatment is symptomatic with pain medication as the condition will typically resolve on its own over several months.Thyroid dysfunction
Thyroid dysfunctionPuneet Shukla
╠²
This document summarizes thyroid dysfunction and diseases. It discusses the basics of thyroid function including production of hormones, control by TSH, and effects of other hormones. It then covers thyroid function tests, diseases including hypothyroidism, hyperthyroidism and thyroiditis, investigations, and management. Key points are TSH and free T4/T3 levels guide diagnosis and treatment with levothyroxine or anti-thyroid drugs depending on hypo- or hyperthyroidism. Thyroid cancer types and appropriate surgery or radioactive iodine treatment are also summarized.Approach to child with short stature
Approach to child with short statureAbdulmoein AlAgha
╠²
A child presenting with short stature should have their height, weight, growth velocity, parental heights, dysmorphic features, pubertal development, bone age, and appropriate investigations assessed. Key factors include determining if growth is proportionate or disproportionate, calculating mid-parental height and target height for comparison, and evaluating bone age to distinguish constitutional growth delay from other causes. A thorough history, physical exam, and targeted laboratory tests can help identify underlying causes like genetic syndromes, malnutrition, endocrine disorders, or chronic illnesses.Short stature in childhood: Challanges & choices (Source: nejm, july 2013)
Short stature in childhood: Challanges & choices (Source: nejm, july 2013)Endocrinology Department, BSMMU
╠²
The document discusses the diagnosis and management of short stature in children, focusing on a case study of an 11.5-year-old boy whose height has significantly decreased percentile-wise. It reviews treatment options including growth hormone therapy and oxandrolone, outlining their efficacy, costs, and potential risks, while emphasizing the importance of individualizing treatment goals based on psychosocial factors. Recommendations include reassessment for those with mild short stature and consideration of low-cost treatment options if psychological distress is evident.More Related Content
What's hot (20)
Cushing syndrome
Cushing syndromeAnitha Dsouza
╠²
Cushing's disease is a hormonal disorder characterized by prolonged exposure to elevated cortisol levels, often caused by benign tumors or excessive use of cortisone medication. Symptoms include obesity, rounded face, muscle wasting, and increased susceptibility to infections, among others. Diagnosis involves various tests, and treatment may include surgery, medications to suppress cortisol production, and management of associated health issues.Puberty normal and precocious
Puberty normal and precociousAbdulmoein AlAgha
╠²
Additional important history:
- Family history of precocious or early puberty
- Developmental milestones
- Medications/supplements
Examination:
- Bone age X-ray
- Pelvic/abdominal ultrasound
- MRI brain
Differential diagnosis:
- Central precocious puberty
- Peripheral precocious puberty (e.g. McCune-Albright syndrome)
- Pseudoprecocious puberty
Investigations:
- LH, FSH, estradiol
- Chromosome analysis
- MRI to rule out CNS pathology
Final diagnosis: Central precocious puberty likely due to early activation of hypDelayed puberty ppt
Delayed puberty pptYassin Alsaleh
╠²
This document provides information on evaluating and treating delayed puberty. It defines delayed puberty and discusses the main causes, which include constitutional delay of puberty, hypogonadotropic hypogonadism, and hypergonadotropic hypogonadism. Evaluation involves assessing medical history, physical exam including Tanner staging, lab tests of hormone levels, bone age, and imaging if needed. Treatment depends on the underlying cause, and may include observation, sex hormone therapy, or treating any underlying medical conditions.Male Hypogonadism
Male HypogonadismSiti Nurul Afiqah Johari
╠²
Male hypogonadism is caused by androgen deficiency which can negatively impact organ functions and quality of life. The goal of testosterone replacement therapy is to restore hormone levels to the normal range and alleviate symptoms. Common treatment options include injections, patches, gels, and implants which can restore sexual function, muscle strength, and bone density. Therapy requires monitoring for side effects like prostate issues or blood clots. Gonadotropins may also be used to stimulate testosterone production and spermatogenesis in hypogonadotropic hypogonadism.Disorder Of Puberty
Disorder Of Pubertydavinpratama
╠²
1) Puberty is the biological changes and sexual maturation that occur during the transition from childhood to adulthood, with the average age of onset being 10-13 years for girls and 12-15 years for boys.
2) Precocious and delayed puberty are disorders defined by puberty onset more than 2 standard deviations outside typical ages. Evaluation of puberty issues includes medical history, physical exam focusing on growth and sexual development, and basic lab tests.
3) Common causes of delayed puberty include constitutional delay, chronic illnesses, nutritional deficiencies, and hormonal disorders; while precocious puberty can be gonadotropin-dependent or -independent. Health care providers must provide long-termPuberty
PubertyAbdulmagid Sarhan
╠²
1) Puberty is the process of physical maturation from child to adult, triggered by hormonal changes. It involves growth, development of secondary sex characteristics, and reproductive ability.
2) The timing of puberty is influenced by genetics as well as environmental factors like nutrition and geography. It typically occurs between ages 8-13 in girls and 9-14 in boys.
3) Precocious puberty describes the onset of puberty before age 8 in girls and age 9 in boys. It can be caused by genetic conditions, brain abnormalities, or tumors and requires medical evaluation and sometimes treatment to delay puberty.Female sex hormones
Female sex hormonesShipra Jain
╠²
This document provides information about estrogens including their biosynthesis, mechanisms of action, pharmacological actions, therapeutic uses, and adverse effects. It discusses natural and synthetic estrogens as well as selective estrogen receptor modulators. Key points include that estradiol is mainly produced in the ovaries and adrenals and acts by binding to nuclear estrogen receptors. Estrogens have various effects in the female reproductive system as well as secondary sex characteristics, bone, brain, liver, and cardiovascular system. Therapeutic uses include hormone replacement therapy and contraception, while adverse effects include an increased risk of certain cancers.Thyroid Hormone
Thyroid HormoneAbdul Wahab
╠²
The document discusses the anatomy, production, regulation, actions, and disorders of the thyroid gland and thyroid hormones. It describes how thyroid hormones are produced in the thyroid gland, transported through the blood, and regulate metabolism and growth through feedback mechanisms involving the hypothalamus and pituitary gland. The summary also discusses hyperthyroidism and hypothyroidism, which can result from excess or deficiency of thyroid hormones.A young boy with signs of puberty
A young boy with signs of pubertyMashfiqul Hasan
╠²
This case discusses a 7-year-old boy presenting with early signs of puberty over the past 5-6 months. Laboratory tests showed elevated levels of testosterone, LH, and FSH, confirming precocious puberty. A GnRH stimulation test showed an LH spike, indicating central precocious puberty. The patient was diagnosed with idiopathic central precocious puberty and prescribed injections of Decapeptyl to delay further pubertal progression until age 11 in order to avoid short adult stature. The document discusses evaluation and management of precocious puberty.Pediatric dosage calculation tutorial 2011(1).ppt
Pediatric dosage calculation tutorial 2011(1).pptJames_Pearce
╠²
This document provides guidance on pediatric dosage calculation, which differs from adult dosage calculation in that doses are based on body weight in kilograms and recommended ranges rather than standard doses. It covers converting weight from pounds to kilograms, writing medication orders, calculating liquid medication doses, reading medication labels, rounding rules, and intravenous drip rates. Practice problems are provided to help learn these concepts.Addison disease
Addison diseaseGagan Velayudhan
╠²
Addison disease is caused by primary adrenocortical deficiency due to destruction of the adrenal cortex, most commonly from autoimmune disease or tuberculosis. It presents with weakness, weight loss, hyperpigmentation, and hypotension due to glucocorticoid and mineralocorticoid deficiency. The diagnosis is made by demonstrating a subnormal response on ACTH stimulation testing with failure to increase cortisol levels above the normal range.Delayed puberty in children
Delayed puberty in childrenAbdulmoein AlAgha
╠²
This document discusses delayed puberty in children. It begins by defining normal puberty and factors that can affect the timing of puberty. It then defines delayed puberty and describes the main types as hypogonadotropic hypogonadism, characterized by low gonadotropins, and hypergonadotropic hypogonadism, characterized by high gonadotropins. The document outlines the evaluation and management of delayed puberty, including history, physical exam, laboratory tests, and treatment approaches depending on the underlying cause. Treatment may involve hormone replacement therapy, addressing underlying medical conditions, or observation in cases of constitutional delay.Puberty dr-arshiyasultana-110312042731-phpapp02
Puberty dr-arshiyasultana-110312042731-phpapp02Asri Purwanti
╠²
Puberty is the transition period between childhood and adulthood that involves physical and hormonal changes. Precocious puberty refers to the onset of puberty before age 8 in girls and age 9 in boys. It can be classified as central, peripheral, or combined based on whether the cause is in the brain or peripheral organs. Diagnosis involves physical exams, hormone tests, imaging, and puberty staging. Treatment depends on the type but may include medication to delay puberty or surgery to remove tumors.Disorders of puberty.pptx 2
Disorders of puberty.pptx 2Whiteraven68
╠²
The document discusses various topics related to puberty, including definitions of key terms, the normal sequence and timing of pubertal changes, causes and treatment of precocious and delayed puberty, and case studies. Precocious puberty can be true/idiopathic, due to tumors or other medical issues, or pseudopuberty caused by medication or conditions like premature adrenarche. Delayed puberty may be due to constitutional delay, medical issues impairing the HPA axis, or prior treatments like radiation therapy. Evaluation and management depends on the underlying cause and aim to initiate puberty normally or replace missing hormones.Normal puberty
Normal pubertyWhiteraven68
╠²
Puberty is the stage of physical maturation triggered by increased secretion of hormones like Luteinizing Hormone and GnRH, resulting in sexual and somatic development. It involves breast development in females starting around age 10-14 and testicular growth in males around age 12-16. Puberty encompasses five stages of physical changes through Tanner stages including growth spurts that make individuals reproductively mature.Addison's Disease
Addison's DiseaseHector Chavez
╠²
Addison's disease is a rare endocrine disorder where the adrenal glands do not produce enough hormones. It is caused by damage to the adrenal cortex, which can be from an autoimmune response, infection, tumors, or other issues. Symptoms include weakness, fatigue, weight changes, and hyperpigmentation of skin. Left untreated, it can cause an Addisonian crisis with severe low blood pressure and other dangerous symptoms. Treatment involves lifelong hormone replacement therapy and monitoring, especially during times of stress. Nursing care focuses on monitoring the patient, educating on treatment and crisis signs, and ensuring fluid and electrolyte balance.Thyroid disorder's
Thyroid disorder'sShubhamSonwane2
╠²
Thyroid disorders can cause the thyroid gland to function abnormally. The document discusses several thyroid disorders including hyperthyroidism (overactive thyroid), hypothyroidism (underactive thyroid), Graves' disease, goiter and thyroiditis (inflammation of the thyroid). It provides details on the causes, symptoms, diagnosis and treatment of these conditions. Thyroid function tests are used to evaluate thyroid function and monitor treatment for thyroid disorders.Precocious puberty
Precocious pubertyKelvin Philip
╠²
1) Precocious puberty is the onset of secondary sexual characteristics before age 8 in girls and age 9 in boys. It can be caused by premature activation of the hypothalamic-pituitary-gonadal axis (central) or premature sex hormone secretion from other sources like the adrenal glands (peripheral).
2) Treatment involves suppressing sex hormone production using GnRH analogues to stop further sexual development and rapid growth. This helps preserve final adult height.
3) Pubertal development is assessed using the Tanner stages, which evaluate breast/genital development and pubic hair growth. Precocious puberty disrupts the normal timing and progression of these stages.Endocrinology thyroid disorder
Endocrinology thyroid disorderLih Yin Chong
╠²
A 27-year-old female presents with palpitations. Exam finds an enlarged, tender thyroid. Labs show suppressed TSH, elevated T4 and low radioactive iodine uptake. The next appropriate test would be to check the ESR, as these findings are consistent with subacute thyroiditis, an inflammation of the thyroid gland often caused by a viral infection. The treatment is symptomatic with pain medication as the condition will typically resolve on its own over several months.Thyroid dysfunction
Thyroid dysfunctionPuneet Shukla
╠²
This document summarizes thyroid dysfunction and diseases. It discusses the basics of thyroid function including production of hormones, control by TSH, and effects of other hormones. It then covers thyroid function tests, diseases including hypothyroidism, hyperthyroidism and thyroiditis, investigations, and management. Key points are TSH and free T4/T3 levels guide diagnosis and treatment with levothyroxine or anti-thyroid drugs depending on hypo- or hyperthyroidism. Thyroid cancer types and appropriate surgery or radioactive iodine treatment are also summarized.Similar to Powerpoint (20)
Approach to child with short stature
Approach to child with short statureAbdulmoein AlAgha
╠²
A child presenting with short stature should have their height, weight, growth velocity, parental heights, dysmorphic features, pubertal development, bone age, and appropriate investigations assessed. Key factors include determining if growth is proportionate or disproportionate, calculating mid-parental height and target height for comparison, and evaluating bone age to distinguish constitutional growth delay from other causes. A thorough history, physical exam, and targeted laboratory tests can help identify underlying causes like genetic syndromes, malnutrition, endocrine disorders, or chronic illnesses.Short stature in childhood: Challanges & choices (Source: nejm, july 2013)
Short stature in childhood: Challanges & choices (Source: nejm, july 2013)Endocrinology Department, BSMMU
╠²
The document discusses the diagnosis and management of short stature in children, focusing on a case study of an 11.5-year-old boy whose height has significantly decreased percentile-wise. It reviews treatment options including growth hormone therapy and oxandrolone, outlining their efficacy, costs, and potential risks, while emphasizing the importance of individualizing treatment goals based on psychosocial factors. Recommendations include reassessment for those with mild short stature and consideration of low-cost treatment options if psychological distress is evident.growthdisorders-141014114149-conversion-gate02.pdf
growthdisorders-141014114149-conversion-gate02.pdfsaadSaad48389
╠²
Growth disorders can cause both short and tall stature. Short stature is defined as height below the 3rd percentile and may be due to familial, genetic, nutritional, endocrine, or environmental factors. Evaluation involves assessing growth velocity, bone age, and screening for underlying causes. Common causes are familial short stature, constitutional growth delay, and growth hormone deficiency. Tall stature is defined as height above the 2 SD line and may be due to genetic factors, growth hormone excess, precocious puberty, or underlying syndromes like Marfan syndrome. Evaluation involves assessing family history and screening for hormonal or metabolic abnormalities.Growth Disorders
Growth DisordersWaleed El-Refaey
╠²
This document provides an overview of growth disorders including short and tall stature. It discusses the evaluation and causes of short stature such as growth hormone deficiency, Turner syndrome, and Prader-Willi syndrome. For growth hormone deficiency, it outlines the diagnostic process including stimulation tests and treatment with growth hormone. For tall stature, it reviews genetic, hormonal, and syndromic causes such as familial tall stature, precocious puberty, and Marfan syndrome.Medicine Tall Stature it's overview & summary
Medicine Tall Stature it's overview & summarySameerAli981890
╠²
Medicine Tall Stature it's overview and it's summary. short stature in children and treatment.pptx
short stature in children and treatment.pptxmaayanaloni
╠²
The document discusses the evaluation and diagnosis of short stature in children, emphasizing the importance of growth monitoring, mid-parental height, and growth velocity assessments. It highlights case studies and diagnostic methods such as bone age measurement and growth hormone tests, ultimately addressing conditions like growth hormone deficiency and its treatment options. It also touches upon idiopathic short stature and the impact of chronic diseases on growth.Short stature a Diagnostic approach
Short stature a Diagnostic approach MohamedRadi19
╠²
1) Short stature is defined as a height more than 2 standard deviations below the average for age and sex. A thorough evaluation considers the child's growth pattern, growth velocity, bone age, medical history, and family history.
2) Basic evaluations include height, weight, bone age, and blood tests. Further testing may include thyroid function tests, serum IGF-1, karyotype, and morning LH/FSH if signs of precocious puberty are present.
3) Causes of short stature include genetic factors, malnutrition, endocrine disorders, chronic diseases, and idiopathic causes. Growth hormone therapy may be considered for growth hormone deficiency, Turner syndrome, and other conditionsAPPROACH AND EVALUATION OF SHORT STATURE.ppt
APPROACH AND EVALUATION OF SHORT STATURE.pptRajenderSingh899217
╠²
The document discusses the approach and evaluation of short stature, focusing on the normal growth pattern influenced by genetic, nutritional, and hormonal factors. It covers prenatal and postnatal growth, mechanisms of catch-up growth, and the pubertal growth spurt, along with various disorders that lead to short stature. Additionally, it provides evaluation strategies for children with short stature, outlining necessary measurements, medical history considerations, and potential interventions.Disorders of growth
Disorders of growthakash chauhan
╠²
Growth disorders include problems that prevent normal development of height, weight, sexual maturity or other features in children. Short stature is defined as a height less than the 3rd percentile or more than 2 standard deviations below the mean for age, sex and population. Common causes of short stature include idiopathic (most common), intrauterine growth restriction, skeletal dysplasias, nutritional deficiencies, and endocrine disorders like growth hormone deficiency. Assessment of a child with short stature involves a detailed history, physical exam, bone age assessment, growth velocity, laboratory tests and sometimes specialized tests or imaging to identify the underlying cause. Management depends on the specific cause but may include dietary interventions, growth hormone therapy, surgery or otherLifespan psychology lecture 5.1
Lifespan psychology lecture 5.1kclancy
╠²
The document provides an overview of physical and psychological changes that occur during adolescence, including:
- Rapid growth and development of primary and secondary sex characteristics due to increases in sex hormones.
- Differences in the timing of puberty between boys and girls, with girls starting earlier on average.
- Changes in body composition with increases in body fat and muscle.
- Brain development continuing into early twenties with improvements in cognitive abilities.
- Health risks such as obesity, eating disorders, drug and alcohol use that can arise during this transitional life stage.Lifespan psychology lecture 5.1
Lifespan psychology lecture 5.1kclancy
╠²
The document provides an overview of physical and psychological changes that occur during adolescence, including:
- Rapid growth and development of primary and secondary sex characteristics due to increases in sex hormones.
- Differences in the timing of puberty between boys and girls, with girls starting earlier on average.
- Changes in body composition with increases in body fat and muscle.
- Brain development continuing into early twenties with improvements in cognitive abilities.
- Health risks such as obesity, eating disorders, drug and alcohol use that can arise during this transitional life stage.Lifespan Psychology Lecture 5.1
Lifespan Psychology Lecture 5.1kclancy
╠²
The document provides an overview of physical and psychological changes that occur during adolescence, including:
- Rapid growth and development of primary and secondary sex characteristics due to increases in sex hormones.
- Differences in the timing of puberty between boys and girls, with girls starting earlier on average.
- Changes in body composition with increases in body fat and muscle.
- Brain development continuing into early twenties with improvements in cognitive abilities.
- Health risks such as obesity, eating disorders, drug and alcohol use that can arise during this transitional life stage.Delayed puberty , etiology , diagnostic approach
Delayed puberty , etiology , diagnostic approach Aftab Siddiqui
╠²
This document provides information on delayed puberty, including its definition, causes, evaluation, and treatment. Delayed puberty can be functional, due to hypogonadotropic hypogonadism, or hypergonadotropic hypogonadism. The most common cause is constitutional delay of growth and puberty. Evaluation involves medical history, physical exam, lab tests like LH, FSH and bone age. Treatment depends on the underlying cause, but aims to induce normal pubertal development and growth. For constitutional delay, watchful waiting is often recommended, while permanent hypogonadism requires hormone therapy like testosterone to initiate puberty.Presentation on Approach to short stature.pptx
Presentation on Approach to short stature.pptxNarayanaLunavath1
╠²
The document discusses short stature, highlighting its definitions, classifications, and the importance of monitoring growth in children. It outlines the criteria for diagnosing short stature, including height percentiles, growth velocity, and potential underlying medical issues. Additionally, it emphasizes the necessity for comprehensive evaluation and appropriate interventions when short stature is identified.Short Stature and Poor Growth - Westchester Health Pediatrics
Short Stature and Poor Growth - Westchester Health PediatricsWestchester Health Pediatrics
╠²
The document discusses the evaluation and causes of short stature and poor growth in children, highlighting the criteria for when intervention is necessary. It outlines the physiological mechanisms involved, such as growth hormone and IGF-1 functions, and presents various causes including nutritional, psychosocial, and medical conditions. Additionally, it provides guidelines for height prediction and the importance of a comprehensive evaluation including medical history and appropriate tests.Evaluation of short stature
Evaluation of short statureKamrul Hasan (Ranga)
╠²
Family seeks medical attention for their short child. The document discusses evaluation of short stature including criteria for pathological short stature, factors regulating growth, assessment of growth including height measurements and bone age, common causes of short stature like constitutional delay of growth and puberty, primary growth hormone deficiency, and hypothyroidism. Evaluation of a short child involves history, physical exam, laboratory tests, and assessing height, parental heights, and bone age.Short stature
Short statureSaptharishi Ganesan
╠²
This document provides an overview of short stature and approaches to evaluating a child presenting with short stature. It defines different types of short stature including familial short stature, constitutional delay of growth and puberty, endocrine causes like growth hormone deficiency and hypothyroidism, disproportionate short stature due to conditions like achondroplasia, chromosomal disorders, emotional deprivation, nutritional causes, and chronic diseases. It also discusses evaluating growth parameters, genetic potential, bone age, causes of short stature, and the role and issues with growth hormone therapy.Short stature Dr.M.Sucindar
Short stature Dr.M.SucindarSucindar M
╠²
This document discusses short stature in children, defining it as height below 2 standard deviations for age and gender. It outlines factors that can affect height, including nutrition, hormones, and intrauterine growth. Short stature is classified as dysmorphic, proportionate, or disproportionate. Evaluation involves medical history, physical exam, auxiliary tests like bone age and growth hormone stimulation, and considering familial, constitutional, nutritional, endocrine, and genetic causes. Management depends on the underlying etiology and may include counseling, dietary changes, surgery, hormone replacement, or growth hormone therapy.Precocious Puberty
Precocious Pubertyranga0007
╠²
Precocious puberty refers to the onset of sexual maturation before age 8 in girls and age 9 in boys. Common signs in girls include breast development, pubic hair growth, growth spurts, and menstruation. In boys, signs are enlargement of the testes or penis, pubic hair growth, growth spurts, and voice deepening. The causes can include brain injuries, infections, thyroid issues, or primary sex organ abnormalities. Treatment involves lowering sex hormone levels with medications like LHRH to stop further sexual development. Supporting the child emotionally is also important.Approach to short stature ppt.pptx
Approach to short stature ppt.pptxRaheelAhmed210939
╠²
Short stature in children is defined as height that is two standard deviations below the mean for age and sex, necessitating regular measurements for accurate assessment. Etiological factors include genetic disorders, chronic illnesses, and nutritional deficiencies, while management involves proper measurement, dietary support, and potential growth hormone treatment. Key considerations for diagnosis include growth velocity and a variety of physical examinations to identify associated syndromes.Short stature in childhood: Challanges & choices (Source: nejm, july 2013)
Short stature in childhood: Challanges & choices (Source: nejm, july 2013)Endocrinology Department, BSMMU
╠²
Powerpoint
- 1. Growth Surendra K. Varma, M.D. University Distinguished Professor and Vice-Chairman of Pediatrics Professor of Physiology and Health Organization Management Residency Program Director Department of Pediatrics
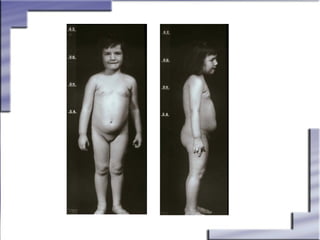
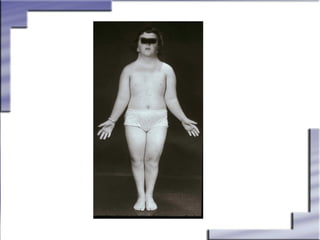
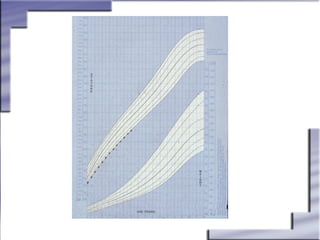
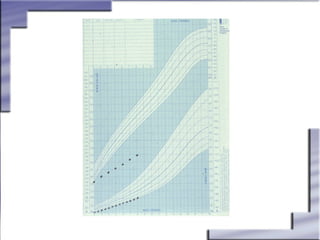
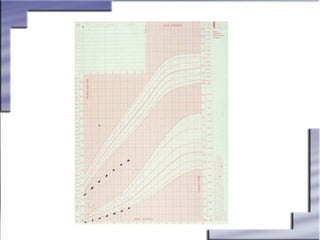
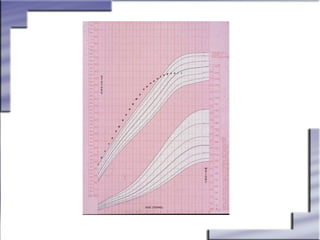
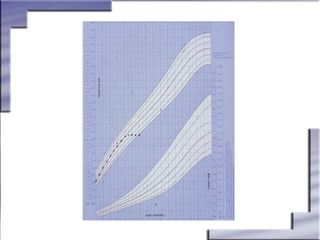
- 6. Assessment of Growth Questions to Ask Parents ’üČIs the child one of the shortest members of the class? ’üČIs the child wearing last yearŌĆÖs clothes? ’üČIs the child growing less than 2 inches per year? ’üČHas the child complained about his or her height? ’üČIs the child unable to keep up with others of the same age at play? ’üČDoes the child show signs of early sexual development? (Before 8 years in girls and before 9 years in boys) ’üČDoes a 13-year-old girl or 15-year-old boy fail to show sings of puberty?
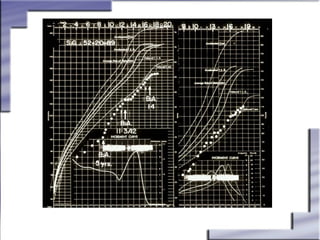
- 7. Assessment of Suspected Growth Abnormalities INITIAL DIAGNOSTIC APPROACH Considerations ’üČPregnancy history ’āśIntrauterine growth retardation (IUGR) ’āśAsphyxia or other birth trauma ’āśToxins (eg. Alcohol, drugs, cigarettes, etc) ’üČGeneral history ’āśChronic illness or debilitating disease ’āśPsychosocial assessment ’üČGrowth history ’āś Height and weight charted (if available, growth velocity) ’üČFamily history ’āśParental stature ’āśMidparental height ’āśParental pubertal patterns
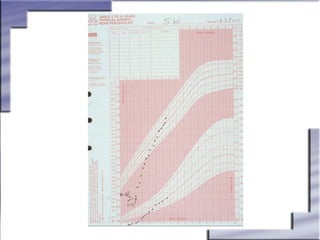
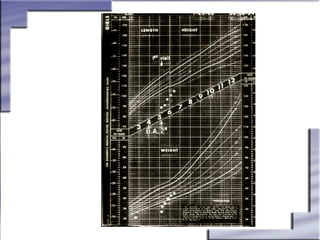
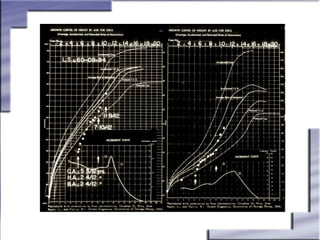
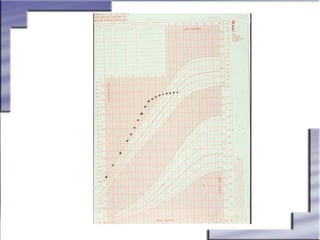
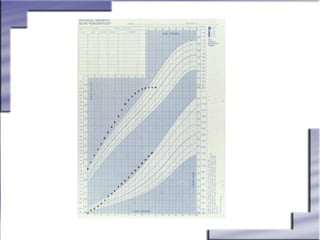
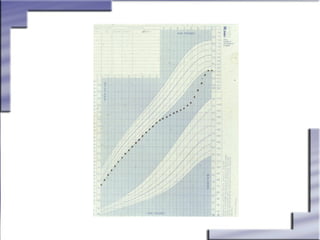
- 8. Assessment of Suspected Growth Abnormalities AUXOLOGIC DATA ’üČAbnormally slow growth rate ’āśAges 3 to 12 years: Less than 2 inches/year (5 cm/year) ’üČDownwardly crossing centile channels on growth chart after the age of 18 months ’üČHeight below third percentile (-2 SD) ’üČHeight significantly below genetic potential (-2 SD below midparental height)
- 9. Growth and Growth Disorders Calculating Target Heights Midparental Height: Girls Boys (F + M) ŌĆō 13 cm 2 (F + M) ŌĆō 13 cm 2 F = fatherŌĆÖs height (cm) M = motherŌĆÖs height (cm) Target Height = Midparental Height + 1.88 SD (1 SD ŌĆō 5cm)
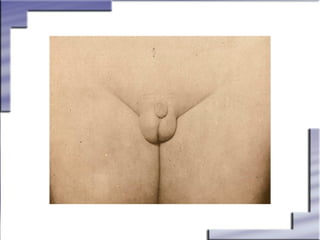
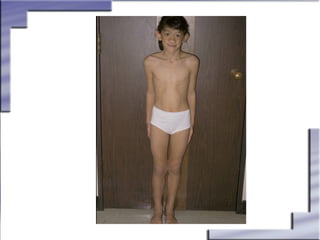
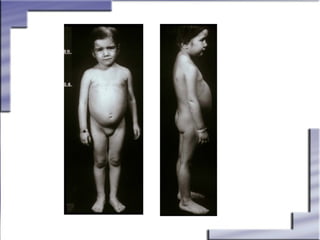
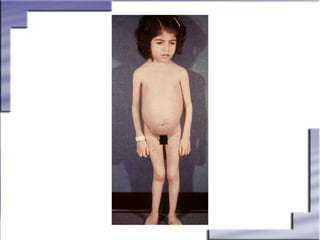
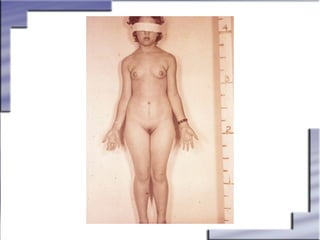
- 10. Assessment of Suspected Growth Abnormalities Physical Examination ’üČHeight and weight accurately measured and plotted ’üČHead circumference recorded ’üČBody proportions assessed ’āśUpper:lower segment ratio ’üČPubertal status ’üČSyndrome-associated features
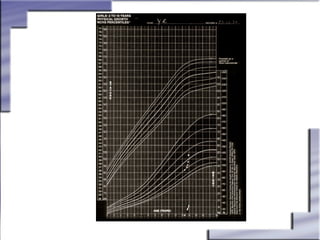
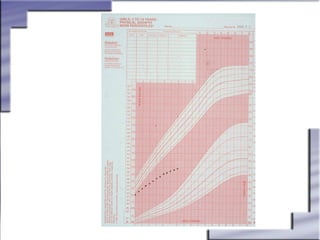
- 11. Assessment of Growth Common Errors at Time of Measurement ’üČFailing to record data ’üČUsing inappropriate growth chart ’üČTransposing height and weight ’üČFailing to plot at closest month/year of age ’üČOmitting of measurements
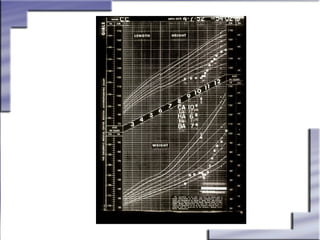
- 12. Assessment of Growth Monitoring Growth ’üČObtain accurate measurements at regular intervals ’üČPlot correctly on appropriate growth chart ’üČDetermine need for further evaluation ’üČGive equal attention to both sexes
- 13. Growth and Growth Disorders Diagnostic Workup Initial Screening Tests ’üČ Complete blood cell count (CBC) ’üČ Erythrocyte sedimentation rate (ESR) ’üČ Blood chemistries, including electrolytes ’üČThyroid profile (L-thyroxine [T4] and thyrotropin [TSH]) ’üČ Kidney profile (urinalysis [UA], blood urea nitrogen [BUN], creatinine) ’üČ Bone age (BA)
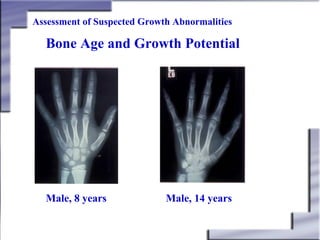
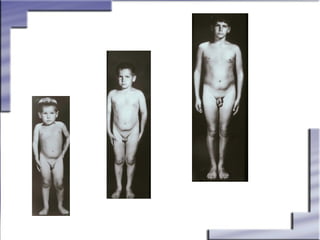
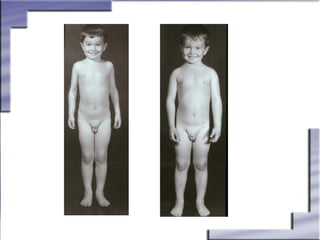
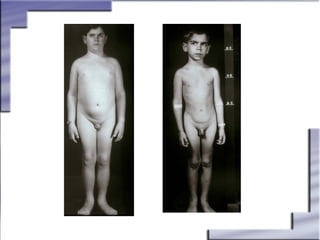
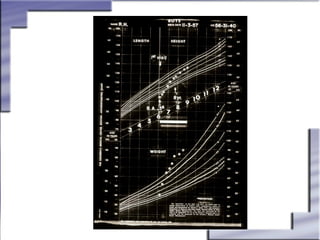
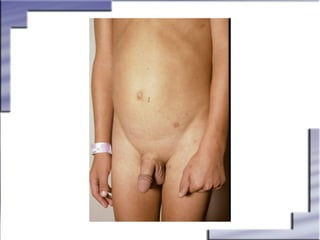
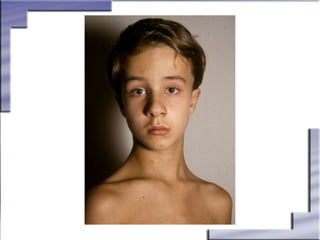
- 14. Assessment of Suspected Growth Abnormalities Bone Age and Growth Potential Male, 8 years Male, 14 years
- 15. Growth and Growth Disorders Diagnostic Workup (cont.) Specialized Tests ’üČChromosomal analysis (karyotype) ’üČIGF-1 and IGFBP-3 ’üČMagnetic resonance imaging (MRI) or computed tomography (CT) studies of the brain
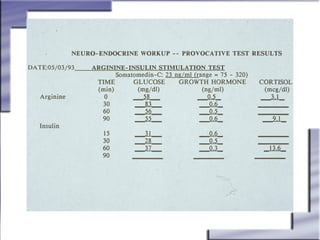
- 18. Differential Diagnosis of Growth Abnormalities Assessment of Growth Hormone Secretion Provocative stimuli ’üČArginine-insulin ’üČClonidine ’üČL-dopa + propranolol ’üČGlucagon ’üČOthers Physiologic tests ’üČExercise-stimulated ’üČSerial sampling
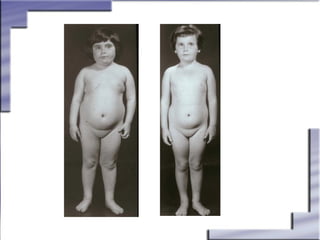
- 19. Growth and Growth Disorders Endocrine Causes of Short Stature ’üČHypothyroidism ’üČHypopituitarism ’üČGlucocorticoid excess ’üČGH insensitivity (Laron syndrome) ’üČEarly exposure to sex steroids ’üČPrecocious puberty ’üČPoorly controlled diabetes mellitus
- 22. Growth Hormone Therapy Historical Perspective ’üČHuman growth hormone (hGH) ’āśFirst available in the 1960s ’āśLimited supplies from cadavers ’āśPossible viral contamination
- 31. Growth and Growth Disorders History of Growth Hormone Therapy for Short Stature ’üČFrom 1950s to 1985, the only treatment available for short stature was cadaveric pituitary hGH ’üČCreutzfeldt-Jakob disease (CJD) reported with cadaveric pituitary hGH ’āśIn 1985, 4 US cases identified ’āśFrom 1985 to 1993, 45 cases reported worldwide ’āśIn 1993, use of cadaveric pituitary hGH banned worldwide ’üČIn 1985, first GH product, Protropin (somatrem for injection) became available
- 32. Growth Hormone Therapy Current Perspective ’üČBiosynthetic growth hormone ’āś Large-scale production made possible by recombinant DNA technology ’āś Highly purified product ’āś Supplies sufficient to treat all GH-inadequate children ’āś Uninterrupted treatment ’āś Precludes contamination
- 33. Differential Diagnosis of Growth Abnormalities Growth Hormone Deficiency ’üČOther systemic causes of short stature ruled out ’üČAfter 3 years of age, subnormal growth rate usually less than 2 inches/year (5 cm/year) ’üČHeight progressively declining to a lower percentile ’üČDelayed bone age ’üČPoor or low response to stimulation testing
- 34. Growth Hormone Therapy Candidates for GH Therapy GH inadequacy ’üČ Demonstrated GH inadequacy with at least 2 stimulation tests ’üČ Subnormal growth velocity for age ’üČ Bone age film indicates growth potential remaining ’üČ All other etiologies ruled out
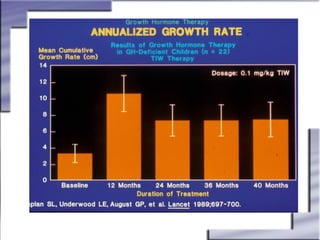
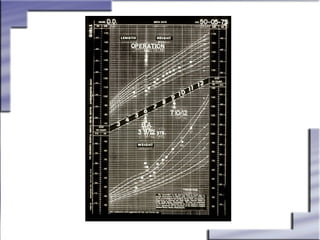
- 35. Growth Hormone Therapy Treatment of GH Inadequacy ’üČInitiate treatment as early as possible ’üČTreatment by subcutaneous injections 3 to 7 times per week ’üČAvoid therapeutic ŌĆ£vacationsŌĆØ ’üČPretreatment growth rate of 3 to 4 cm/year accelerates to 8 to 10 cm/year during the first year ’üČTreatment continues until satisfactory height achieved or epiphyseal fusion occurs
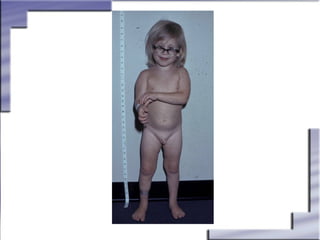
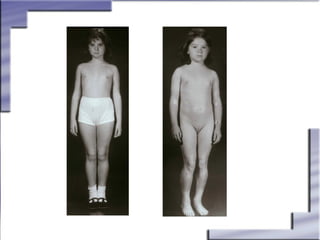
- 47. Potential Application of GH Therapy Role of Growth Hormone Therapy in the Treatment of: ’üČTurner syndrome ’üČChronic renal insufficiency ’üČIdiopathic short stature
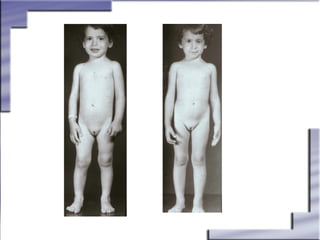
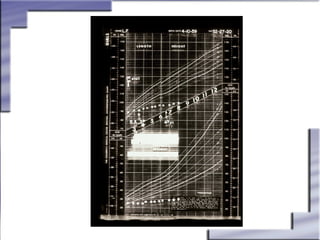
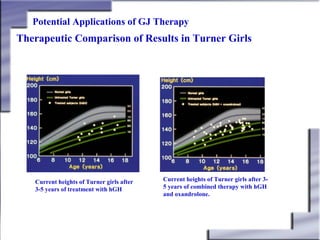
- 49. Potential Applications of GJ Therapy Therapeutic Comparison of Results in Turner Girls Current heights of Turner girls after 3-5 years of treatment with hGH Current heights of Turner girls after 35 years of combined therapy with hGH and oxandrolone.
- 62. Growth and Growth Disorders Non-endocrine Systemic Disorders Affecting Growth ’üČRespiratory disease ’āśAsthma ’āśCystic fibrosis ’üČRenal disease ’āśHypoplastic kidneys ’āśRenal tubular acidosis ’āśChronic renal insufficiency ’üČHematologic disease ’āśChronic anemias
- 63. Growth and Growth Disorders Non-endocrine Systemic Disorders Affecting Growth ’üČGastrointestinal disorders ’āśInflammatory bowel disease ’āśChronic liver disease ’āśCeliac disease ’āśCystic fibrosis ’āśOther malabsorption diseases ’üČMalnutrition ’üČDiabetes mellitus ’üČCardiac diseases