Primary survey in Trauma
•Download as PPTX, PDF•
129 likes•60,993 views

1) A 25-year-old male was in a high-speed head-on collision as an unrestrained driver and is unresponsive upon arrival with abnormal vital signs and injuries. 2) During the primary survey, the team will follow the ATLS protocol to simultaneously assess and treat the patient's airway, breathing, circulation, disability, and exposure (ABCDEs). 3) Adjuncts like diagnostic tools, vital sign monitoring, and urinary/gastric catheters will be used as needed during primary survey and resuscitation before proceeding to secondary survey and definitive care, with continuous re-evaluation of the stabilized patient.























Primary survey in Trauma
- 1. Initial assessment Primary survey Dr Vinod Jain
- 2. Objectives • To understand the ATLS principles during primary survey • To know the application of adjuncts
- 3. Case scenario • 25 years old male, unrestrained car driver with high speed head-on collision, brought by police ambulance • HR 110/mt, RR 32/mt, BP 100/80, Pale skin • Unresponsive with alcoholic smell • Bleeding wound right thigh and left hand with deformity • Noisy breathing • Bruises on anterior chest wall
- 4. Case scenario • Should be managed by single person or by a team? • Is it important to assign work to different team members? • Prior basic information of patient’s condition is helpful or not?
- 5. Case scenario What is the sequence of priorities in assessing this patient? • Should we identify the specific injuries before initial management of this patient? • If not, how should we proceed?
- 6. ATLS way of trauma management • Preparation • Triage • Primary survey (ABCDEs) • Resuscitation • Adjuncts to primary survey and resuscitation • Secondary survey • Adjuncts to secondary survey • Continuous post resuscitation monitoring and re evaluation • Definitive care
- 7. Preparation • Take universal precautions • Check the availability of medicines and functioning of equipments • Designate the role to each team member • Utilize pre hospital information
- 8. Initial assessment • Primary survey – Evaluates physiology • Secondary Survey – Evaluates anatomy
- 9. Primary survey Primary survey and resuscitation of vital functions are done simultaneously using a team approach
- 10. Primary Survey – ATLS way • Airway with c-spine protection • Breathing and ventilation • Circulation with hemorrhage control • Disability: Neuro status • Exposure with environmental control
- 11. Primary Survey Always consider physiological variations in special populations â—Ź Elderly â—Ź Infants and Children â—Ź Pregnant Women â—Ź Obese â—Ź Athletes The priorities are same for all the patients
- 12. Quick Assesment What is a quick, simple way to assess a patient in 10 seconds? • Ask the patient his or her name? • Ask the patient what happened?
- 13. Appropriate Response confirms 1 – Patent airway 2 – Sufficient air reserve to permit speech 3 – Sufficient perfusion 4 – Clear sensorium
- 14. Primary survey Airway – Establish patent airway with c-spine protection • Clear the airway using wide bore suction • Chin lift / Jaw thrust manoeuvre • Oropharyngeal / nasopharyngeal airway • Definitive airway (Cuffed, Secured endotracheal tube) • Surgical airway
- 15. 15
- 16. Primary Survey Breathing and ventilation – assess and ensure adequate oxygenation and ventilation
- 17. Breathing and Ventilation Assess • Jugular venous distension • Position of trachea • Respiratory rate • Percussion findings of chest • Air entry • Oxygen saturation
- 18. Breathing and ventilation Recognise and treat early – • Tension pneumothorax • Flail chest with pulmonary contusion • Massive haemothorax • Open pneumothorax Immediate Chest decompression with Oxygen delivery
- 19. Circulation with haemorrhage control After excluding tension pneumothorax, cause of hypotension is hypovolemia until proved otherwise
- 20. Circulation with haemorrhage control Look for blood loss – External bleeding – Internal bleeding • Chest • Abdomen / Retroperitoneum • Pelvis • Long bones One on floor four more
- 21. Circulation with haemorrhage control Assess for organ perfusion â—Ź Level of consciousness â—Ź Skin color and temperature â—Ź Pulse rate and character
- 22. Primary Survey Circulatory Management â—Ź Control hemorrhage â—Ź Restore volume â—Ź Reassess patient Pitfalls â—Ź Elderly â—Ź Children â—Ź Athletes â—Ź Medications
- 23. D- Disability : Neurologic status Rapid neurological examination is done for - - Level of consciousness (GCS) - Pupillary size and reaction - Localizing signs
- 24. Primary survey - E • Expose the patient • Prevent hypothermia • Cover with warm blanket Patient’s body temperature is more important than comfort of healthcare providers
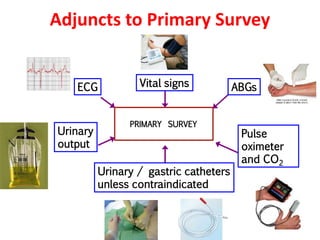
- 26. Adjuncts to Primary Survey PRIMARY SURVEY ABGs Urinary / gastric catheters unless contraindicated Urinary output ECG Vital signs Pulse oximeter and CO2
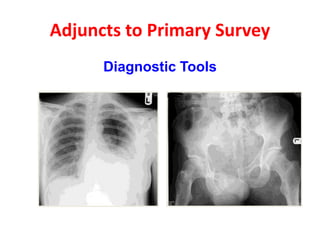
- 27. Adjuncts to Primary Survey Diagnostic Tools
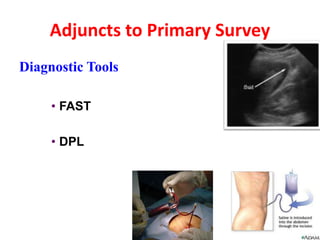
- 28. Adjuncts to Primary Survey Diagnostic Tools • FAST • DPL
- 29. Parameters of improvement Normalization of • Pulse rate • Blood pressure • Ventilatory rate • Arterial blood gases (ABG) • Body temperature • Urinary output
- 30. Transfer • Consider transfer after stabilization
- 31. Transfer protocol Inform the receiving doctor about • Patient’s history including mechanism • Physical findings • Treatment instituted • Patient’s response to therapy • Diagnostics tests performed and result • Need for transport • Method of transportation • Anticipated time of arrival Continue ABCDEs with continuous monitoring
- 32. Questions
- 34. Take home message • We should have competent and co-ordinated team for trauma care • Correct and sequential ATLS approach is needed • Primary survey includes simultaneous assessment and treatment of trauma patient • Priorities of resuscitation remain same in various population of trauma patients • Proper transfer protocol should be followed