
























Probiotics
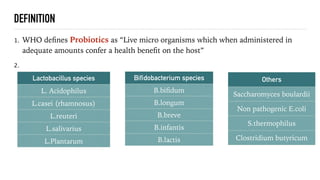
- 2. DEFINITION 1. WHO deïŽnes Probiotics as âLive micro organisms which when administered in adequate amounts confer a health beneïŽt on the hostâ 2. Lactobacillus species L. Acidophilus L.casei (rhamnosus) L.reuteri L.salivarius L.Plantarum Bifidobacterium species B.biïŽdum B.longum B.breve B.infantis B.lactis Others Saccharomyces boulardii Non pathogenic E.coli S.thermophilus Clostridium butyricum
- 3. MECHANISMS OF BENEFIT 1. BeneïŽts of probiotics are incompletely understood 2. Suppression of growth or epithelial binding/invasion by pathogenic bacteria 3. Improvement of intestinal bacterial function 4. Modulation of the immune system 5. Modulation of pain perception
- 4. 1. Some of the commercially available probiotics include: 2. VSL#3 (BiïŽdobacterium breve,B.longum,B.infantis,Lactobacillus acidophillus,L.plantarum,L.paracasei,L.bulgaricus,streptococcus thermophilus) 3. Align(B.infantis) 4. Culturelle(L.rhamnosus GG) 5. DanActive(L.casei) 6. MutaïŽor(E.coli Nissle 1917) 7. Florastor(s.boulardii)
- 5. CHARACTERISTICS OF EFFECTIVE PROBIOTICS 1. Able to survive the passage through the digestive system 2. Able to attach to the intestinal epithelial and colonise 3. Able to maintain good viability 4. Able to utilise the nutrients and substrates in a normal diet 5. Non pathogenic and non toxic 6. Stability of desired characteristics during processing,storage and transportation 7. Anti-inïŽammatory,antimutagenic,immunostimulatory
- 6. MICROBIOTA AND MICROBIOME 1. Healthy adult harbours~ 100 trillion bacteria in gut alone 2. This is 10x the number of human cells we possess 3. Humans possess 23,000 genes 4. Microbiota contributes ~33,00,000 5. Communal gut microbial genome (microbiome) is ~150 times larger than human genome 6. Is dominated by 4 large groups of bacteria or phyla: Actinobacteria,Bacteroidetes,Firmicutes,Proteobacteria
- 11. 1. Bacteria express glycoside hydrolyse which converts glycans into useable sugars 2. No enzyme encoded in human genome is capable of digesting glycans -only bacterial enzymes 3. Many carbohydrates are digestible only by bacteria and produce SCFA-primary fuel for colonocytes 4. 10-15% of adult energy may be generated by SCFA production
- 14. 1. PREBIOTICS- Nondigestable carbohydrates that stimulate the growth and activity of beneïŽcial colonic bacteria 2. Best source of prebiotic ïŽber are Inulin and oligosaccharides(fructooligosaccharides and galactooligosaccharides) 3. Traditional dietary sources of PREBIOTICS include soybeans,raw oats,unreïŽned wheat and barely 4. When these are metabolised by gut microbes,short chain fatty acids are produced 5. SCFs nourish cells that line the gut 6. Reduces the risk for cancer in the gut 7. Enhance calcium absorption and relieve constipation and diarrhoea 8. SYNBIOTICS- Mixture of Pro and PREBIOTICS
- 15. DIET INFLUENCES MICROBIOME COMPOSITION Long term diet is associated with development of speciïŽc Enterocytes 1. Diets high in animal protein and fat with high levels of Bacteroides and low levels of Prevotella 2. Diets high in carbohydrates but low in animal protein and fat with higher levels of prevotella butvlower levels of Bacteroides Japanese harbour organisms that produce enzyme that aids in sea weed digestion Microbiota of African children enriched in Bacteroides and depleted in Firmicutes to maximize energy uptake from ïŽbre rich diet.
- 18. REVERSING DYSBIOSIS 1. Colectomy 2. Colon cleaning 3. Antibiotics 4. Prebiotics 5. Probiotics 6. Faecal transplantation
- 19. ALLERGIC DISEASES 1. Studies have shown diïŽerences in the early colonisation patterns of infants who develop allergic disease 2. Low levels of BiïŽdobacterium and early colonisation with potentially pathogenic bacteria,such as Clostridioides(formerly clostridium) diïŽcile and staphylococcus aureus, were more prevalent in children who subsequently developed allergy 3. High diversity of Microbiota is required for immune system maturation,which is less in allergic patients 4. World Allergy organisation suggests use of PREBIOTICS only in infants who are not exclusively breastfed and probiotics in pregnant and lactating women and in infants when there is high risk of allergy in the children
- 20. 1. CONSTIPATION- Improvement in defecation frequency ,stool consistency,and intestinal transit time with BiïŽdobacterium lactis DN-173 010,B.lactis BB12,Lactobacillus casei Shirota,L.reuteri DSM 19738 and E.coli Nissle 1917. 2. Should be avoided in management of severe constipation in elderly and in children with functional constipation 3. PANCREATITIS- Probiotics did not reduce the risk of infectious complications and actually increased mortality from mesentric ischemia. 4. LACTOSE INTOLERANCE: Lactose fermenting Lactobacillus acidophilus strain showed reduced symptoms after in vivo lactose challenge
- 21. DIARRHEAL ILLNESSES 1. Infectious diarrhoea- May be considered for use in children and adults.It reduces the duration of diarrhoea 2. In acute rotavirus diarrhoea in children ,VSL#3 signiïŽcantly decreased stool frequency. 3. Lactobacillus GG showed a dose dependent decrease in fecal shedding of rotavirus 4. Protective mechanisms include strengthening the mucosal barrier,blocking viral entry,decreased viral toxin expression,and inducing antiviral IgA. 5. A combination of seven Lactobacillus,BiïŽdobacterium, and streptococcus thermophilus signiïŽcantly decreased acute dysentery bleeding and hospitalisation. 6. Celiac diseases- No evidence to support the use of probiotics in patients with celiac disease
- 22. Clostridioides(formerly clostridium) diïŽcle infection 1. Probiotics when given with antibiotics,there is 60% risk reduction in development of clostridium diïŽcle associated diarrhoea 2. No enough evidence to support use of probiotics in treating clostridium diïŽcile infection 3. Pouchitis-Study of patients with pouchitis showed persistence of Fusobacteria and enteric species,increased clostridium perfringens,and the absence of streptococcus species 4. VSL#3 found more eïŽective for preventing relapse of chronic pouchitis and prevention onset of pouchitis
- 23. FECAL TRANSPLANTATION 1. First performed in 1958 for fulminant pseudomembranes 2. Now accepted as eïŽective for recurrent C.diïŽcile 3. 92% eïŽective when standard therapy failed 4. Administered by NG,NJ,enema or colonoscopy 5. EïŽcacy slightly improved with antibiotics before Microbiota transplantation
- 24. INFLAMMATORY BOWEL DISEASE 1. Various probiotic species have shown promise in the treatment of ulcerative colitis,but these studies are done in small no of patients and no strong conclusions in systematic reviews 2. E. coli 1917 Nissle was shown to be as eïŽective as low dose 5-ASA in preventing relapse 3. Lactobacillus GG appeared to be more eïŽective than standard treatment involving mesalazine in prolonging relapse free time,but did not inïŽuence relapse rates 4. Combination of a prebiotic and a probiotic(B.longum) was associated with improvement in histological scores 5. Crohn disease- Available data do not support clinical eïŽectiveness of probiotic therapy for either induction or maintenance of remission
- 26. NEXT GENERATION PROBIOTICS 1. These come from the human intestinal microbes and include novel bacteria that have not been previously used as health promoting agent. 2. L.reuteri produces an antibacterial compound from glycerol called reuterin and this can eliminate clostridium diïŽcile. 3. It has also got antibiotic resistance properties,so this can be used in recurrent c.diïŽcile infection in addition to antibiotics