
![ïï Skin
o Rash only during fever (JIA)
o No sweat (familial dysautonomia)
o Petechiae (endocarditis, rickettsia)
o Papules (cat scratch)
o Eschar (tularaemia)
o Erythema migrans (Lyme)
o Malar (SLE)
o Palpable purpura [polyarteritis nodosa (PAN)]
o Erythema nodosum (JIA, SLE, streptococcal, infection, malignancy, IBD, TB)
o Seborrheic dermatitis(histiocytosis)
o Sparse hair (ectodermal dysplasia)](https://image.slidesharecdn.com/puobydraabdurrazaqalt-190924173452/85/PUO-18-320.jpg)


PUO
- 1. PUO Guideline by Dr A Abdurrazaq
- 2. Definition : Fever of unknown origin refers to the presence of a documented fever for a specified time, for which a cause has not been found after a basic medical evaluation.
- 3. History Fever: -Thermometer used , - its type, - factitious, - site , - core or peripheral
- 4. Pattern: ïą Continuous: Temperature remains above normal throughout the day and does not fluctuate more than 1 °C in 24 hours (meningitis, encephalitis, Lobar pneumonia, typhus fever).
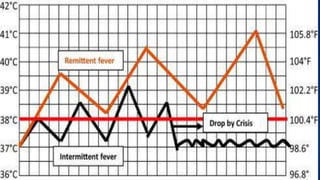
- 5. ïą Remittent: Temperature remains above normal throughout the day and fluctuates more than 1 °C in 24 hours ( Endocarditis,brucellosis).
- 6. ïą Intermittent: Temperature elevation is present only for a certain period, later cycling back to normal ( Tertian fever in Plasmodium vivax , ovale & falciparum. Quartan fever in P. malariae, TB , JIA ),
- 7. Another class of intermittent fever is Pel-Ebstein fever weeks high for one week and low for the next week and so on
- 8. ïą Undulant Fever: Rising & falling like a wave (Brucellosis)
- 9. ïą Cyclical fever: usually every 3 weeks (cyclic neutropenia & Hyper IgD ).
- 11. Height & Duration: Temperature below 38.5 intermittent is usually due to Viral infection .Temperature above 40 is a pediatric emergency.(Infectious causes: septicaemia,ruseola, measles. Non infectious: Kawasaki disease, malignant hyperthermia, drug fever ,rarely intracranial Hge).
- 12. Response to: paracetamol and or NSAID (no response: dysautonomia)
- 13. Associated symptoms: ïķ Nasal discharge(Sinusitis), ïķ Red eyes(Kawasaki ), ïķ GI ( IBD ,Salmonella,Abcesses), Recurrent pharyngitis with ulcers ( Periodic fever) in people of Mediterranean origin (FMF), ïķ Salmon rash only during fever (JIA), ïķ Limb pain (leukaemia, osteomyelitis,JIA
- 14. Other part of the history: ïï History of travel to TB-endemic region (Pakistan,India,china ,Nigeria,) Malaria endemic regions (central & south America, Haiti, Africa). ïï Prophylaxis & immunization ïï History of contact with cat, sheep, dog, monkey o Bites (tick: arbovirus, malaria) o Meat: undercooked (brucella,toxoplasma, hepatitis) o Pica (visceral larva migrans, toxoplasmosis)
- 15. ï Drug history: All including non -prescription (Drug fever), Antibiotics eg cephalosporin, penicillin, Phenytoin can all cause drug fever. ï Ethnicity: Sephardic Jew, Armenian, Turkish, Arab (Familial Mediterranean Fever), Ashkenazi Jew (Riley-Day Syndrome).
- 16. Examination: ïï ENT: o Sinuses o Lymphadenopathy (Malignancy, EBV, CMV) o Red, no exudates (EBV) o Dental abscess o Conical teeth (ectodermal dysplasia) o Smooth tongue (dysautonomia) o Gum hypertrophy, tooth loss(leukaemia, histiocytosis).
- 17. ïï Eyes: o Conjunctivitis o palpebral (infectious mononucleosis) o bulbar (Kawasaki) ,Phlyctenular (TB) o Retinopathy (PAN, miliary TB, toxoplasmosis, vasculitis) o Pupil dilation (hypothalamic or autonomic dysfunction)
- 18. ïï Skin o Rash only during fever (JIA) o No sweat (familial dysautonomia) o Petechiae (endocarditis, rickettsia) o Papules (cat scratch) o Eschar (tularaemia) o Erythema migrans (Lyme) o Malar (SLE) o Palpable purpura [polyarteritis nodosa (PAN)] o Erythema nodosum (JIA, SLE, streptococcal, infection, malignancy, IBD, TB) o Seborrheic dermatitis(histiocytosis) o Sparse hair (ectodermal dysplasia)
- 19. ïï Chest & Cardiovascular: o Murmur (Endocarditis or left atrial myxoma) o Crackles(lobar pneumonia) ïï Abdominal: o Hepato/spleno-megally(salmonella, cat scratch, endocarditis, malaria), o point tenderness (Intra-abdominal abscess). ïï Genito-urinary: o Girls â Pelvic tenderness (child sex abuse â STI)
- 20. ïï Musculo-skeletal: ïą Tender: - Bone (osteomyelitis, malignancy) - Muscle (trichinella,arbovirus,dermatomyositis) - Trapezius (subdiaphragmatic abscess) ïą Reflexes: - Brisk (hyperthyroid) - Absent (dysautonomia)
- 21. Investigation: ï Basic Investigation: FBC, ESR, CRP, U&E, LFT, blood culture, urinalysis, urine & stool culture, CXR,X-ray sinus cavities
- 22. ï 2nd line Non âinvasive Investigations: o Viral cultures, o Serology for (brucellosis,weil felix for rickettsia,widal test for salmonella, leptospiral & herpes group viruses) o ANA,C3,C4 , C-ANCA ,Ig G,A,M,D, &E levels with subsets, o TB Quantiferon. o USS (Abdo,pelvic ,chest & lymph node). o EBV & CMV titres. o Ophthalmologist review
- 23. ï Selective Investigations: o CT or MRI (Abdo & Head) , o Bone scan , o Tissue, lymph node or bone marrow biopsy. o ECHO, o PCR for HIV, o DNA analysis for fabrys disease . o PET Scan , o White cell scan.
- 24. ï Management: ïą Empirical Antibiotics : Ceftriaxone or cefotaxime if critically ill or fever in less than 3 months. ïą TB treatment after lymph node biopsy, induced sputum or TB sputum culture. ïą Overall it is good practice to avoid antibiotics until an organism is isolated.
- 25. Referral - Gastroenterologist âIBD , - Rheumatology âJIA ,CTD -Oncologist- Leukemia - Cardiologist-Endocarditis, Left atrial Myxoma - ID â TB, Brucellosis, Salmonella, HIV