












Rectus muscle hematoma management protocol.ppt
- 2. is an anticoagulant normally used in the prevention of thrombosis , thromboembolism and the formation of blood clots in the blood vessels and their migration elsewhere in the body. It was referred to as a "blood thinner", this is a misnomer, since it does not affect the viscosity of blood . Warfarin
- 3. Mechanism of action Warfarin inhibits the vitamin K-dependent synthesis of biologically active forms of the calcium dependent clotting factors II , VII, IX and X, as well as the regulatory factors protein C, protein S .
- 4. Indications of wafarin • Deep-vein thrombosis. • Pulmonary embolism • Atrial fibrillation which is risk of embolisation. • Mechanical prosthetic heart valves (to prevent emboli developing on the valves).
- 5. *It is essential that the INR be determined daily or on alternate days in early days of treatment, then at longer intervals (depending on response) then up to every 12 weeks. Monitoring * Baseline INR is recommended prior to initiating warfarin therapy to assess sensitivity . * An INR within the last 48 hours is acceptable as a current baseline INR . * With initial dosing, the INR will usually increase within 24- 36 hours .
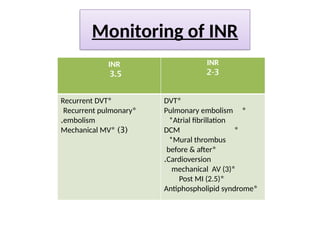
- 6. Monitoring of INR INR 3.5 INR 2-3 * Recurrent DVT * Recurrent pulmonary embolism . ( 3 * ) Mechanical MV * DVT * Pulmonary embolism *Atrial fibrillation * DCM *Mural thrombus * before & after Cardioversion . * mechanical AV (3) * Post MI (2.5) * Antiphospholipid syndrome
- 7. Warfarin toxicity is common and usually results from dose changes or drug interactions .
- 8. Presentations of warfarin toxicity Major bleeding e.g. : * : 1) hemorrhage * GI hemorrhage * intracranial bleeding * retroperitoneal bleeding *Minor bleeding e.g. : * mucous membranes * subconjunctival hemorrhage * hematuria *epistaxis, and ecchymoses
- 9. Follow))Presentations of warfarin toxicity 2 ) Skin necrosis: usually observed between the third and eighth days of therapy, is a relatively uncommon . It may require treatment through debridement or amputation of the affected tissue . It occurs more frequently in women and in patients with preexisting protein C deficiency .
- 10. Follow))Presentations of warfarin toxicity : 3 ) Osteoporosis The mechanism was thought to be a combination of reduced intake of vitamin K, which is necessary for bone health, and inhibition by warfarin of vitamin K-mediated carboxylation of certain bone proteins, rendering them nonfunctional .
- 11. Follow))Presentations of warfarin toxicity 4 ) Purple toe syndrome : It is another rare complication that may occur early during warfarin treatment (usually within 3 to 8 weeks of commencement). This condition is thought to result from small deposits of cholesterol breaking loose and flowing into the blood vessels in the skin of the feet, which causes a bluish purple color and may be painful . It is typically thought to affect the big toe, but it affects other parts of the feet as well, including the bottom of the foot (plantar surface). The occurrence of purple toe syndrome may require discontinuation of warfarin .
- 12. Follow))Presentations of warfarin toxicity : 5 ) Drug interactions Here some medications affect INR : INR Depression INR Elevation rifampicin amiodarone secobarbital ciprofloxacin carbamazepine Metronidazole , fluconazole phenytoin Clarithromycin . erythromycin Phenobarbital fluvastatin , lovastatin primidone fluvoxamine Cigarette smoking isoniazide phenylbutazone
- 13. Natural Products That Can Alter the Anticoagulant Effect of Warfarin Decreased Anticoagulant Effect Increased Anticoagulant Effect Alfalfa Asafetida , Clove Oil Ginseng Garlic ,Ginger Ginseng ,Anise
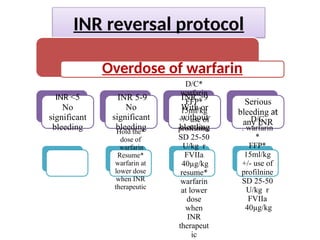
- 14. INR reversal protocol Overdose of warfarin INR <5 No significant bleeding INR 5-9 No significant bleeding * Hold the dose of warfarin * Resume warfarin at lower dose when INR therapeutic INR >9 With or without bleeding * D/C warfarin * FFP 15ml/kg +/- use of profilnine SD 25-50 U/kg r FVIIa 40µg/kg * resume warfarin at lower dose when INR therapeut ic Serious bleeding at any INR D/C warfarin . * * FFP 15ml/kg +/- use of profilnine SD 25-50 U/kg r FVIIa 40µg/kg
- 15. Thank you