



Respiratory Disease
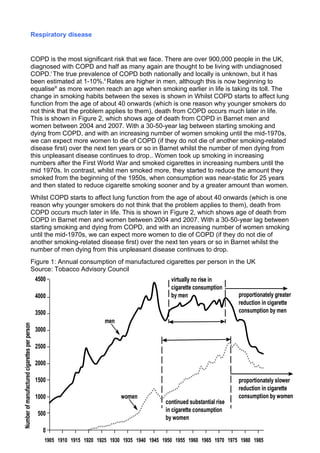
- 1. Respiratory disease COPD is the most significant risk that we face. There are over 900,000 people in the UK, diagnosed with COPD and half as many again are thought to be living with undiagnosed COPD.i The true prevalence of COPD both nationally and locally is unknown, but it has been estimated at 1-10%.ii Rates are higher in men, although this is now beginning to equaliseiii as more women reach an age when smoking earlier in life is taking its toll. The change in smoking habits between the sexes is shown in Whilst COPD starts to affect lung function from the age of about 40 onwards (which is one reason why younger smokers do not think that the problem applies to them), death from COPD occurs much later in life. This is shown in Figure 2, which shows age of death from COPD in Barnet men and women between 2004 and 2007. With a 30-50-year lag between starting smoking and dying from COPD, and with an increasing number of women smoking until the mid-1970s, we can expect more women to die of COPD (if they do not die of another smoking-related disease first) over the next ten years or so in Barnet whilst the number of men dying from this unpleasant disease continues to drop.. Women took up smoking in increasing numbers after the First World War and smoked cigarettes in increasing numbers until the mid 1970s. In contrast, whilst men smoked more, they started to reduce the amount they smoked from the beginning of the 1950s, when consumption was near-static for 25 years and then stated to reduce cigarette smoking sooner and by a greater amount than women. Whilst COPD starts to affect lung function from the age of about 40 onwards (which is one reason why younger smokers do not think that the problem applies to them), death from COPD occurs much later in life. This is shown in Figure 2, which shows age of death from COPD in Barnet men and women between 2004 and 2007. With a 30-50-year lag between starting smoking and dying from COPD, and with an increasing number of women smoking until the mid-1970s, we can expect more women to die of COPD (if they do not die of another smoking-related disease first) over the next ten years or so in Barnet whilst the number of men dying from this unpleasant disease continues to drop. Figure 1: Annual consumption of manufactured cigarettes per person in the UK Source: Tobacco Advisory Council 4500 virtually no rise in cigarette consumption proportionately greater by men 4000 reduction in cigarette consumption by men 3500 men Number of manufactured cigarettes per person 3000 2500 2000 1500 proportionately slower reduction in cigarette consumption by women women 1000 continued substantial rise in cigarette consumption 500 by women 0 1905 1910 1915 1920 1925 1930 1935 1940 1945 1950 1955 1960 1965 1970 1975 1980 1985
- 2. In Barnet, death rates from COPD are reducing faster in men than they are in women, as shown in Figure 2 and we can expect this gender difference to continue for some time. Figure 2: Trends in age-standardised death rates from COPD in Barnet in men and women Source: Office for National Statistics 45 Age-standardised death per 100,000 40 Men Women 35 30 25 20 15 10 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 Figure 3 shows the total number of men and women dying from lung cancer in Barnet. This also indicates that 30-40 years ago, women were more likely to start smoking at an older age than men. As women now tend to take up smoking in their early teens, as men used to, we can expect women to die at a younger age from lung cancer than they do now. Stopping smoking is important whatever the degree of disability someone has because of COPD. This has two important effects: it prevents the damage getting worse and it reduces the risk of hospitalisation. Research has shown that stopping smoking more than halved the likelihood of hospital admission, but merely reducing smoking does not make any significant difference.iv The risk of people suffering and dying from other respiratory diseases can also be reduced by quitting smoking â it increases oneâs likelihood of developing acute bronchitis â and, for those in at-risk groups, of having an annual influenza immunisation. Asthma is predominantly a cause of intermittent breathing difficulty and a relatively unusual cause of death. For most people, it can be wholly managed in a primary care setting with only a small number requiring hospital admission for severe attacks.
- 3. Figure 3: Total number of deaths from COPD in men and women in Barnet 2004-2007 50 45 40 Men 35 Women 30 25 20 15 10 5 0 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89 90+ Source: Office for National Statistics The relationship between diversity and deprivation and respiratory disease There is a relationship between respiratory disease and deprivation. Figure 4 shows the hospital admission rate for respiratory disease in 2006/07 for residents in each of Barnetâs electoral wards ranked in order of deprivation. In most instances, there is a close and increasing relationship between the two: people living in more deprived areas are more likely to have respiratory disease that is severe enough to require hospital admission. It is noteworthy that smoking is more prevalent in more deprived areas. There are insufficient data currently available to indicate any relationship between ethnicity or other aspects of diversity and respiratory disease. However, it is likely that different smoking habits in men and women in different ethnic groups is likely to have an effect on this. Figure 4: The relationship between hospital admission for respiratory disease and deprivation 30 Admission rate per 1000 population 25 20 15 10 5 0 10 12 14 16 18 20 22 24 26 28 30 32 34 Index of Multiple Deprivation 2007 Source: Local hospital admission data Local targets
- 4. Currently, there is no formal target to reduce death rates from respiratory disease. However, reducing deaths from respiratory diseases of all types will contribute to reducing the all-age, all-cause death rate and, with appropriate targeting of activity, contribute to reducing health inequalities. Key things that need to be done The key activities required are: continuing to reduce the prevalence of smoking; ïŪ continuing to encourage and enable the uptake of influenza immunisation and ïŪ pneumococcal immunisation; the provision of services to manage acute exacerbations of COPD early and to provide ïŪ pulmonary rehabilitation services.
- 5. i Soriano JB, Maier WC, Eager P, et al. Recent trends in physician diagnosed COPD in women and men in the UK. Thorax 2000;55:789-94 ii British Thoracic Society Standards of Care Subcommittee on Pulmonary Rehabilitation. Pulmonary Rehabilitation. Thorax 2001;56:827-834 iii Calverley P. COPD: early detection and intervention. Chest 2000; 117:S365-S371 iv Godtfredsen NS, Vestbo J, Prescott E Risk of hospital admission for COPD following smoking cessation and reduction: a Danish population studyâ Thorax 2002, 57:967-972