Reverse cold chain
âĒDownload as PPTX, PDFâĒ
4 likesâĒ7,589 views

This document discusses the reverse cold chain process for maintaining the cold temperature of samples collected from acute flaccid paralysis (AFP) cases that are transported from clinics to laboratories for poliovirus testing. Key aspects of the reverse cold chain include standards for sample collection, storage and transport at 0-8°C, as well as reporting criteria to document the absence of poliovirus circulation. Innovations include using temperature log tags to track specimens and providing incentives for reporting AFP cases.













Reverse cold chain
- 1. REVERSE COLD CHAIN Presented by: Palka Mittal Sahdev Bishnoi M.Voc. (Public Health)
- 2. CONTENT âĒ INTRODUCTION âĒ NEED OF REVERSE COLD CHAIN âĒ SURVEILLANCE STANDARDS âĒ CLASSIFICATION SCHEME âĒ STANDARDS FOR SAMPLE COLLECTION âĒ STORATGE AND TRANSPORT CONDITIONS âĒ REPORTING CRITERIA âĒ INNOVATIONS
- 3. Reverse Cold Chain The process of maintaining the cold chain when heat sensitive items are stored and transported in the reverse direction i.e. upward from the clinic to a depot or laboratory.
- 4. Reverse Cold Chain-WHO âIf a cold chain is what you call the transport chain that goes from a laboratory to the field â where vaccines must be kept at a certain temperature from the moment they are produced, until they are administered in order for them to work â a reverse cold chain is the process of stool samples that need to be tested getting back to the laboratory from the field at certain temperatures so that the virus that might be in the sample will still be identifiable.â
- 5. Why reverse cold chain? âĒ Poliomyelitis is targeted for eradication. Highly sensitive surveillance for acute flaccid paralysis (AFP), including immediate case investigation, and specimen collection are critical for documenting the absence of poliovirus circulation for polio-free certification âĒ When any case of acute flaccid paralysis is found anywhere in the world, stool samples from the affected child must be transported carefully to the laboratory so that they can be tested to identify whether the poliovirus was the cause.
- 6. Surveillance Standards of Poliomyelitis As per WHO Clinical case definition âĒ Any child under 15 years of age with AFP* or any person of any age with paralytic illness if polio is suspected Case classification âĒ Suspected case: A case that meets the clinical case definition âĒ Confirmed case
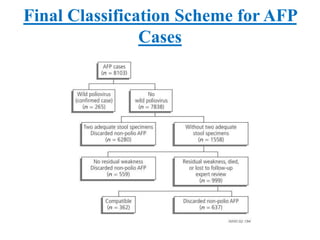
- 7. Final Classification Scheme for AFP Cases
- 8. Standards for Sample collection âĒ Collect two samples 24-48 hours apart and within 14 days of the onset of paralysis âĒ Volume of specimen must be adequate(approximately 8-10g) âĒ Appropriate documentation (i.e. laboratory request form) âĒ Sample must be in good condition, i.e. with no leakage or desiccation âĒ Evidence that the reverse cold chain has been maintained (presence of ice or temperature indicator)
- 9. Specimen-Based Data âĒ Unique identifier âĒ Specimen number: 1 = first specimen; 2 = second specimen; 3 = other; 9 = unknown âĒ Date of onset of paralysis âĒ Date of last OPV dose âĒ Date of collection of stool specimen âĒ Date stool specimen sent to laboratory âĒ Date stool specimen received in laboratory âĒ Condition of stool: 1 = good; 2 = poor; 9 = unknown âĒ Date final culture results sent from laboratory to EPI(Expanded Program on Immunization)
- 10. Rules for Specimen Storage and Transport Poliovirus is sensitive to heat, therefore âĒ After collection, the specimens must be placed immediately in a refrigerator or, for shipment, in a cold box at 0â8°C between frozen ice packs. âĒ Aim for the specimens to arrive at the laboratory within 72 hours of collection. âĒ If this is not possible, the specimens must be frozen (at -20°C) and then shipped frozen, preferably with dry ice or with cold packs that have also been frozen at - 20°C. âĒ Try to limit repeated freezing and thawing to a minimum. This process of keeping the specimen refrigerated or frozen is called a âreverse cold chainâ.
- 11. Remember âĒ Avoid storing samples in refrigerators or cold boxes used for vaccines or medicines. âĒ If separate storage is unavoidable, seal specimens in 2-3 layers of plastic bags and separate them properly from vaccines.
- 12. Diagrammatic Representation (a) 30-60 ml faeces container with external screw cap. (b) Sealed polyethylene bag to hold faeces containers. (c) Sealed polyethylene bag to hold report form. (d) Absorbent material (cotton wool absorbs 8-10 times its own weight). (e) Icepacks obtainable from national EPI. (f) High-density (30-35 kgs/m3) polystyrene (small bubbles and firm when squeezed). (g) Infectious substance label. (h) Outer carton of double-ply corrugated cardboard or plastic.
- 13. Reporting Criteria âĒ Aggregated data on AFP cases should be included in routine monthly surveillance reports âĒ Designated reporting sites at all levels should report at a specified frequency (e.g. weekly or monthly) even if there are zero cases (often referred to as "zero reporting") âĒ All outbreaks should be investigated immediately âĒ All AFP cases under 15 years of age or with paralytic illness at an age where polio is suspected should be reported immediately and investigated within 48 hours âĒ Active surveillance: Regular weekly visits should be made to selected reporting sites that are most likely to admit acute flaccid paralysis patients (e.g. major hospitals, physiotherapy centers) to look for unreported AFP cases
- 14. Innovations in the reverse cold chain âĒ Introduction of continual temperature recording probes known as âLog Tagsâ to track specimens during their journey to the lab. âĒ Incentives are paid for informants who report a case.