



















Rheumatoid arthritis
- 2. GENETICS 1.Allelic variation in HLA-DRB1,especially 0401,0405,0901 in asian ancestry 2.Inheritance of risk allele of PTPN22 3.Polymorphisms of PAD14 ENVIRONMENT 1.Cigarette smoking increases risk 2.EBV viral infection is associated with increased risk for RA
- 3. PATHOPHYSIOLOGY 1.Genetics and environment interaction activates TH cells into TH1 and TH17 2.TH cells will signal macrophages of synovium to secrete TNF ALPHA,IL1,IL6,GMCSF 3.TNF ALPHA upregulates DKK1,which then promotes internalization of WNT receptors into osteoblast precursors which inhibits bone formation 4.Stromal cells and TH cells will express RANKL,which in presence of MCSF binds to RANK on precurser osteoclast. 5.This will convert it to activated osteoclast,which erodes bones.
- 5. CLINICAL FEATURES -Disease of middle aged female. -inflammation of joints,tendons,bursae. - early morning stiffness lasting more than 1 hr,that eases with activity. -small joints of hands and feet are commonly involved,initially mono/oligo/poly articular with symmetric distribution ARTICULAR -WRIST,MCP,PIP are frequently involved joints. -DIP involvement is rare. -FLEXOR TENDON TENOSYNOVITIS is hallmark.
- 6. -ULNAR DEVIATION:From subluxation of MCP -SWAN NECK DEFORMITY:hyperextension of PIP,flexion of DIP -BOUTONNIERE DEFORMITY:Flexion of PIP with hyperextension of DIP. -Z LINE: hyperextension of 1st PIP JOINT,subluxation of 1st MCP. OTHER DEFORMITIES: PIANO KEY MOVEMENT OF ULNAR STYLOID,PESPLANOCAVUS -ATLANTO AXIAL SUBLUXATION,CERVICAL COMPRESSIVE MYELOPATHY may occur.
- 7. EXTRA ARTICULAR 1.CONSTITUTIONAL 2.NODULES: -Subcutaneous nodules seen in 40% patients. - firm,nontendor,seen on areas of skeleton subjected to repeated trauma like forearm,sacral prominences,achilis tendons. 3.SJOGRENS SYNDROME 4.PULMONARY: -Pluiritis -ILD -Pulmonary nodules -caplans syndrome (pulm nodules+pneumoconiosis)
- 8. 5.CARDIAC: -Pericarditis -granulomatous myocarditis -mitral regurgitation 6.VASCULITIS: 7.POLYNEUROPATHY/MONONEURITIS MULTIPLEX 8.HEMATOLOGICAL: -Normocytic,normochromic anemia -felty”s syndrome(neutropenia,splenomegaly,nodular RA) 9.LYMPHOMA ASSOCIATED CONDITIONS- cardio.vd,osteoporosis,hypoandrogenism
- 9. CLINICAL COURSE 1.10% will undergo spontaneous remission in 6 months. 2.Majority will have persistant progressive course with waxing and wanning intensity. 3.Some will have intermittent attacks with quiescency in between. 4.Overall mortality is higher with IHD as a cause,next cause is infections.
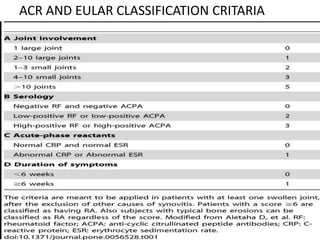
- 10. ACR AND EULAR CLASSIFICATION CRITARIA
- 11. WORK UP 1.ALL ROUTINE INVESTIGATIONS 2.ESR,CRP 3.RF,ANTI CCP Abs 4.SYNOVIAL FLUID :WBC@ 2000-50,000/microL 5.IMAGING: -for diagnosing and tracking progression -X ray,MRI,USG
- 12. X Ray: -periarticular osteopenia -soft tissue swelling,symmetric joint space loss,subchondral erosions -joint subluxation,collapse USG: -detects more erosions than Xray -detects synovitis,other soft tissue changes MRI: -high sensitivity for synovitis and joint effusions -detects bone marrow edema which is early finding of subsequent joint disease.
- 14. INDIVIDUAL DRUGS 1.NSAIDS: -for symptoms -chronic use should be avoided 2.STEROIDS: -to achieve rapid control -as DMARDS take several weeks for onset of disease activity control -and 1-2 weeks course maay be described in acute flares. -if there is no response to DMARDS,then steroids can be added. -if only few joints involved intra-articular stroids can be given,and in ILD. -best practice is to avoid chronic steroids ,if it is inevitable,add bisphosphonates to prevent osteoporosis.
- 15. 3.DMARDS: -DMARDS will slow/prevent progression of structural progression of RA. COVENTIONAL: 1.METHOTREXATE: -its DMARD of choice for RA. -its anchor drug for many combination therapies. DOSE: 10-25 mg/week along with folate 1mg/d SE:hepatotoxicity,myelosupression,infections,intistit ial pneumonitis,teratogenic,nausea diarhrhea,oral ulcers. MONITORING:CBP,LFT,RFT every 2-3 monthly.
- 16. 2.SULFASALAZINE: DOSE-500mg BD,1000-1500 mg/day maintenance. SE: hemolytic anemia with G6P deficiency,granulocytopenia,nause,dairhrhea MONITOR:CBP every 2-3 weeks for first 3 months,then every 3 months. -before starting G6P level. 3.HCQ: -not a true DMARD -used for mild disease and as adjunctive -DOSE: 200-400 mg/d OD. 4.LEFLUNOMIDE:-pyramidine synthesis inhibitor -DOSE:10-20 mg/d , -SE: hepatotoxicity,myelosupression,infections,teratog enic,alopecia
- 17. BIOLOGIC DMARDS: (MNE-RAT) 1.RITUXIMAB: -monoclonal ab agnst CD 20. -useful in refractory RA. -1000 mg/iv on day 0,14.repeat after 24 wks. -SE: infections,infusion reactions,cytopenias,hepatitis B reactivation,PML(Progressive Multifocal Leukoencephalopathy). 2.ANAKIRA: -IL 1 receptor antagonist. -DOSE:100 mg/sc dialy. -SE: Infections,reactivation of TB,Neutropenias
- 18. 3.ABATACEPT: - inhibits costimulation of T cells by blocking CD28-CD 80/86 interactions. DOSE: weight based 60-100 kg—750 mg/iv -at 0,2,4 th week f/b every 4 weks once. SE:Infections 4.TNF ALPHA INHIBITORS: a)infliximab: dose-3mg/kg /iv@ week 0,2,6 then every 8 weeks. b)etenarcept: 50 mg sc weekly c)adalimumab: 40 mg sc alternate weekly e)golimumab: 50 mg sc monthly once f)certolizumab: 400 mg@ 0,2,4 week,f/b alt wkly.
- 19. SE:Infections,reactivation of latent TB,infusion site reactions,raised LFTs,neurological deficits. 5.TOCLIZUMAB: 4-8 mg/iv monthly. -Mab against IL-6 receptor. -SE: infection,infusion reactions,raised LFTs,cytopenias,dyslipidemia. 6.TOFACITINIB: 5mg po BD. -Inhibit JAK1 and JAK3 signalling which mediates IL2,4,7,9,15,21 and IL6,INF gamma. -SE: infection,neutropenia,alterLFT,dyslipidemia, nasopharyngitis,headache,URTI.
- 20. HOW TO PRESCRIBE Goals 1.Early aggressive therapy to prevent joint damage and disability. 2.Using combination therapy where appropriate. 3.Frequent modification of therapy according to response. 4.Individualization of therapy. 5.Achieving remssion.
- 21. 1.Start off with methotrexate and add HCQ,sulfasalazine if no adequate response @ 6 months.(step up strategy) or 2.Start of with oral triple therapy(methotrexate,sulfasalazine,hcq) and add biologic @ 3 months if disease activity still persists or 3.In patients with high initial disease activity biologicals can be started first as combination therapy with other drugs. 4.Remission is goal of therapy.
- 22. HOW TO ASSESS DISEASE ACTIVITY According to EULAR 2 definitions for remission… 1. All of the following a.Tender joint count < 1 b.swollen joint count <1 c.CRP<1 mg/dl d.patient global assessment<1 (0-10 scale) 2.SDAI-INDEX < 3.3
- 23. PHYSICAL THERAPY AND ASSIST DEVICES 1.Dynamic strength training 2.Comprehensive physical therapy 3.Physical activity coaching 4.Foot orthotics 5.Wrist splints SURGERY –for failed medical rx,for deformities 1.Silicone implants 2.Arthrodesis 3.Arthroplasty
- 24. PREGNANCY AND RA 1.Prednisolone,Hcq,sulfasalazine combo is safe 2.contraindicated-methotrexate,sulfaslazine 3.Biologicals have no data in pregnancy so avoid -75% will note improvement during pregnancy -Relapse after delivery ELDERLY -measure RFT and adjust doses accordingly -avoid methotrexate if s.cr >2 mg/dl.