scre3ning of diseases epidemiology community medicine screening.ppt
?Download as PPT, PDF?
0 likes?75 views

Community medicine screening























scre3ning of diseases epidemiology community medicine screening.ppt
- 1. Screening for Disease Dr Meenakshi Khapre
- 3. ¡°LEAD TIME¡± It is the period between diagnosis by early detection and diagnosis by other means. Detection programmes should be restricted to those conditions in which there is considerable time lag between disease onset and the usual time of diagnosis.
- 4. ¡°Screening is the search for unrecognized disease or defect by means of rapidly applied tests, examinations or other procedures in apparently healthy individuals.¡± ¡°Screening includes methods; technique; procedure and examinations for early and rapid detection of unrecognized disease or defect in apparently healthy persons.¡± A screening program tests people for a disease or condition before they have symptoms of the disease. Screening for disease
- 5. Definitions of screening have been changing with time & they range from simplest to most complicated ones, one of which defines it as ¡®It is a medical investigation which doesn¡¯t arise from patient¡¯s request for advice for a specific complaints¡¯ while the latest one by National Screening Committee 2nd report(2000) is ¡®Screening is a public health service in which members of a defined population who do not necessarily perceive that they are at risk of or are already affected by a disease or it¡¯s complications are asked a question or offered a test to identify those individuals who are more likely to be helped than harmed by further tests or treatment to reduce the risk of disease or it¡¯s complications¡¯
- 6. The benefits of screening were 1st introduce by the use of mass miniature radiography (MMR) for the identification of individual with TB. With the introduction of effective treatment for this condition after the second word war. The use of MMR became widespread in many western countries particularly with USA and UK. In the late 1950¡¯s and early 1960¡¯s special campaign of mass radiography were used to good effect in Scotland 1st in Glasgow and then throughout the country to try and find unknown and infection sufferer from TB.
- 7. Screening is carried out in the hope that earlier diagnosis and subsequent treatment favorably alters the natural history of the disease in significant proportion of those who are identified as ¡°positive¡± The goal of this program is to discover conditions in there earliest and most treatable stages. The program only works for certain conditions where there is effective treatment, and effective and sensitive screening tests. In these cases, minimally invasive treatments can be used, and improved life expectancy should result. 1 Control of disease 2 Researches 3 Early diagnoses 4 Educational Purposes
- 8. ? Case detection Also known as ¡®Prescriptive screening¡¯ it is defined as presumptive identification of unrecognized disease which doesn't from patient¡¯s request. ? Control of disease Also known as ¡®prospective screening¡¯ ie people are examined for benefit of others. ? Research purposes Screening may aid in obtaining basic knowledge about natural history of diseases whose etiology/pathogenesis is obscure. ? Educational opportunities Helpful in creating public awareness & educating health professionals.
- 9. Mass Screening It is screening of whole population or a sub group It has gone out of use nowadays. High Risk / Selective Screening It is most productive because it is applied to selectively to the high risk group on the basis of epidemiological research Multi Phasic Screening It is application of two or more screening tests in combination to large no. of people at one time than to carry out separate screening tests for single disease
- 10. Cont¡ ? Multipurpose screening ? Opportunistic screening
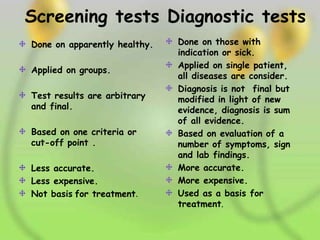
- 11. Screening tests Diagnostic tests Done on apparently healthy. Applied on groups. Test results are arbitrary and final. Based on one criteria or cut-off point . Less accurate. Less expensive. Not basis for treatment. Done on those with indication or sick. Applied on single patient, all diseases are consider. Diagnosis is not final but modified in light of new evidence, diagnosis is sum of all evidence. Based on evaluation of a number of symptoms, sign and lab findings. More accurate. More expensive. Used as a basis for treatment.
- 12. CRITERIA for screening for diseases Criteria acceptable, and safe screening tests are essential; the disease screened must be common and should have a detectable preclinical stage, for which effective treatment should be available; a large proportion of people at risk should participate in screening, investigations and treatment; the local health services infrastructure should be sufficiently developed to provide the diagnostic, treatment and follow-up services.
- 13. Consideration for criteria ? Diseases to be screened ?The tests to be applied
- 14. Diseases to be screened should fulfill the following criteria 1. The condition sought 2. Latent or early asymptomatic stage 3. The natural history of condition 4. Facilites available to confirm diagnosis 5. Effective treatment 6. Policy to treat Early detection & treatment reduces morbidity & mortality.
- 15. Screening tests to be applied The test must satisfy the criteria of acceptability, repeatability, validity besides others like yield,simplicity, safety,rapidity,ease of adsministration & of cost.
- 16. Screening test 1.Acceptability The test should be acceptible to all the peoples at whom it is aimed. 2.Reapeatability The test must give consistent results when repeated more than once on same individual or material under same condition.It depends upon 3 major factors.
- 17. Screening test ? 3 factors on which repeatability depends upon are 1.Observer variation (a)Intra observer variation (b)Inter observer variation 2.Biological variation 3.Errors related to technical methods
- 18. Repeatability 1.OBSERVER VARIATION All observations are subjected to variation. ? If a single observer takes 2 measurements in the same subject,at the same time & each time,he obtained a different result it is termed as intra-observer variation. ? The variation between different observers on the same subject or material is called inter- observer variation.
- 19. Repeatability ? 2.Biological variation It is assotiated with physiologic variables such as blood pressure,blood sugar etc. Fluctuation is due to changes in the parameters obs,variations in the way the patient percive their sympt & ans & regression to the mean. ? 3.errors related to technical methods Repeatability may be affected by variations inherent in the methods.
- 20. Screening test ? 3.validity It refers to what extent the test accurately measures which it purports to measure. Eg: glycosuria is a useful test for screening for diabetes,but a more valid test is the glucose tolerence test. It has two components sensitivity & specificity.
- 22. Evaluationof screeningtests Following measures are used to evaluate a screening test : Sensitivity Specificity Predictive value of a positive test Predictive value of a negative test Percentage of false negative Percentage of false positive
- 23. Sensitivity The term was introduced by Yerushalmy in 1940¡¯s. it is define as the ability of a test to identify correctly all those who have the disease. i.e. true positive. Specificity It is define as the ability of a test to identify correctly those who do not have disease i.e. ¡°true negative¡±. Predictive accuracy It reflects diagnostic power of the test. Predictive value of a positive test reflects the probability that a patient with a positive test result has in fact the disease in question. The more prevalent a disease is in a given population, the more accurate will be the predictive value of a positive screening test .
- 24. False negatives & False positives The term false negatives means that the patient who actually have the disease are told that they do not have the disease. It amounts to giving them false reassurance. False positives It means that patients who do not have the disease they are told they have. In this case normal people are subjected to further investigations at some inconvenience, discomfort, anxiety & expense. They not only are burden to diagnostic facilities but they also bring discredit to screening programme
- 25. Summary of criteria for evaluation of screening ? Factors ? Simplicity ? Acceptibility ? Accuracy ? Cost ? Repeatability ? Sensitivity ? Specificity ? Criteria ? Simple to perform easy to interupt & paramedical person should be able to perform. ? It must be acceptable to all who are undergoing it ? It should give true measurements of condition or symptom ? Expense of test must be considered in relation of early detection of disease ? The test should give consistent result in repeated trials ? The test should be capable of giving a positive finding when individual being is screened has condition being sought ? Test should be capable of giving negative results when individual being screened doesn¡¯t condition being sought
- 26. Yield It is the amount of previously unrecognized disease that is diagnosed as a result of the screening efforts. It depends upon many factors ¨C Sensitivity & specificity of the test, prevalence of the disease, the participation of individuals in the detection programme. Hence to enhance the yield high risk population are usually selected. Higher the Yield, higher is the efficiency of screening programme. Combination of tests Two or more tests can used in combination in order to enhance the efficiency of screening
- 27. The Problem Of Borderline ? The question arises which of the two qualities (sensitivity or specificity) is more important in screening? ? (a) Bimodal distribution.The two curves overlap.The shaded area will comprise a mixture of persons with diseases & persons without diseases. ? (b) Unimodal distribution.No line dividing between the ¡°normal¡± & ¡°diseased¡±.
- 28. Decision Making Prior decision is made about the cut-off point. The following factors are taken into consideration. (a) DISEASE PREVALENCE: When the prevalence is high in the community,the screening level is set at a lower level. (b) THE DISEASE: IF the disease is very lethal (e.g;cervical cancer,breast cancer) and early detection markedly improves