2. Introduction
’ü¼ According to WHO, around 100 million of
people are patients of diabetes in the world.
Diabetes deaths are likely to increase by more than 50% in the next 10
years without urgent action.
3. Diabetes will be a primary killer
WHO and IDF indicates that 3.2 million deaths
happen for diabetes in each year. In the
world about 6 deaths occur in every minutes
for diabetes. Diabetes a primary cause of
kidney failure, blindness, and amputations
and so why it said that, in next 25 years
diabetes will be the one primary killer.
.
.
4. Diabetes
’ü¼ Definition from WHO:
-Diabetes mellitus is a metabolic disorder of
multiple etiology which is characterized by
chronic hyperglycemia with disturbance of
carbohydrate, fat and protein metabollism
resulting from defects of insulin secretion,
insulin action or both.
5. Effect of diabetes
’ü¼ long term damage.
’ü¼ Dysfunction.
’ü¼ Failure of different organ.
6. Causes
’ü¼ Impaired glucose intake by skeletal muscle.
’ü¼ Impaired glycogenesis.
’ü¼ Impaired hepatic output of glucose.
’ü¼ Impaired input of glucose.
7. Symptoms of diabetes
’ü¼ Classical symptoms are-
*Thirst
*Polyuria
*Weight loss
*Blurred vision
But in severe form ŌĆō
*Develop ketoacidosis because of fat breaking.
*Non ketonic hyperosmolar state will increase. This
will lead to coma, if untreated it leads to death.
8. Classification of Diabetes
’ü¼ Diabetes Mellitus (DM) is classified as ŌĆō
1) Type-1 Diabetes Mellitus
2) Type-2 Diabetes Mellitus
9. Type-1 Diabetes Mellitus
Insulin Dependent Diabetes Mellitus or
Juvenile Diabetes. It results from pancreatic
Beta cell destruction and severe in insulin
deficiency. It occurs mostly in Juvenile but
occasionally at adults, specially the non-
obese.
10. Type-2 Diabetes Mellitus
’ü¼ Non-Insulin Dependent Diabetes Mellitus,
occurs in adult. It is characterized by tissue
resistance to the action of insulin combined
with a relative deficiency of insulin. Although
insulin is produced by Beta cell it is
inadequate to overcome the resistance and
blood glucose rises.
11. Some other types
’ü¼ MRDM: Malnutrition Related Diabetes
Mellitus.
’ü¼ GDM: Gestational Diabetes Mellitus.
12. Treatment
’ü¼ Many complications of diabetes can be
prevented or delayed through effective
management. This includes ŌĆō
* Healthy diets.
* Physical activity.
* Avoidance of over weights and obesity.
* Not smoking.
13. Treatment
’ü¼ Diabetes therapy is not only about lowering
glucose level but also about the overall
complications such as blood pressure and
blood lipids. This requires life long care and
management.
’ü¼ People with type 2 diabetes often require oral
drugs and sometimes insulin is used to
control their blood levels.
15. Insulin
’ü¼ Insulin is a small protein which contains two
chains (A and B) linked by disulfide bridges.
Insulin is released from pancreatic B cells at
a low basal rate and at much higher
stimulated rate in response to a variety of
stimuli, especially glucose.
16. Chemistry of insulin
’ü¼ It consists of two open poly-peptide chains (A
and B). There are 21 amino acids in chain A
and 30 amino acids in B chain. Two chains
are inter-linked by a di ŌĆō sulfide bridge. There
is an additional disulfide bridge between the
6th
and 11th
amino acid residues of the A
chain. Breaking the di ŌĆō sulfide bridge,
inactive insulin. It is protein in nature. ItŌĆÖs MW
is 5800.
18. Pharmacokynetics of insulin
’ü¼ Route of administration : Subcuteneous, IV,
IM.(orally insulin is digested because it is
protein in nature).
’ü¼ Adsorption : slow in subcuteneous.
’ü¼ Metabolism : Liver 60%, Kidney 40%.
’ü¼ Plasma half life : 3 ŌĆō 9 minutes.
’ü¼ Excretion : Urine.
19. Hyperglycemia
’ü¼ Hyperglycemia is a condition in which blood
sugar increases above the normal level, i.e.
above 120mg per 100ml. When the blood
sugar level exceeds the renal threshold,
sugar appears in the urine. It mainly occurs
due to the ŌĆō
* Impaired glucose intake by skeletal muscle.
21. Hypoglycemia
’ü¼ Hypoglycemia is a condition in which blood sugar
decreases below the normal level e. i. below 40mg
per 100ml. The symptoms ŌĆō
* Sweating
* Anxiety
* Dizziness
* Headache
* Weakness
* Fall in blood pressure.
22. Hypoglycemic agent
’ü¼ Hypoglycemic agents are the agents which
used in the treatment and prevention of
diabetes mellitus. They are capable of
reducing blood sugar level.
23. Glycosuria
’ü¼ It is the condition when the glucose reuptake
by the kidney is impaired. In this condition
blood glucose level exceeds 80mg glucose
per 100ml of blood.
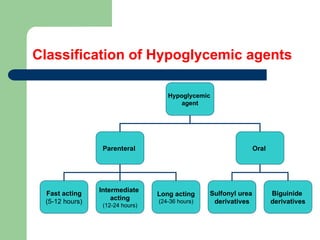
24. Classification of Hypoglycemic agents
Hypoglycemic
agent
Parenteral Oral
Sulfonyl urea
derivatives
Biguinide
derivatives
Fast acting
(5-12 hours)
Long acting
(24-36 hours)
Intermediate
acting
(12-24 hours)
28. Sulfonyl urea
’ü¼ Chemistry
Sulfonylureas are chemically related with
sulfonamide structure.The compounds are
aryl-sulfonyl-ureas with substitution on the
benzene and urea group.The basic structure
is-
R1 SO2 ŌĆōNH-CO-NH-R2
R1 SO2 ŌĆōNH-CO-NH-R2
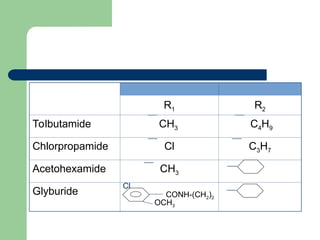
29. SAR of Sulfonylureas
’ü¼ Activity and potency of sulfonylureas change
with introducing of new group or substituents
to the basic structure of sulfonylureas called
SAR of sulfonylureas.
R1 SO2 ŌĆōNH-CO-NH-R2
31. Mechanism of action
’ü¼ The main action of sulfonylureas is to
stimulate the Beta cells of islets of
langerhans, causing insulin secretion and
thus reducing plasma glucose.
’ü¼ High affinity receptors for sulfonylureas are
present on the K-ATP channels in Beta cell
plasma membrane and the binding of various
sulfonylureas parallels their potency in
stimulating insulin release.
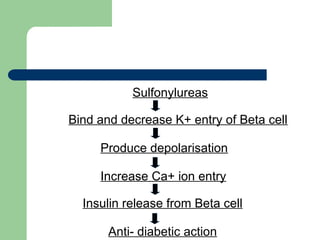
32. Sulfonylureas
Bind and decrease K+ entry of Beta cell
Produce depolarisation
Increase Ca+ ion entry
Insulin release from Beta cell
Anti- diabetic action
33. Pharmacokynetics
’ü¼ Route of administration : Oral.
’ü¼ Absorbtion : Absorbed well from the gut with
food.
’ü¼ Distribution : 99% protein bound, can cross
placenta.
’ü¼ Metabolism : Liver.
’ü¼ Excretion : Urine.
35. Contraindications
’ü¼ Diabetes in pregnancy.
’ü¼ Known allergy to drug.
’ü¼ IDDM.
’ü¼ After surgery.
’ü¼ Severe renal insufficiency and hepatic
failure.
’ü¼ Elderly patient with impaired renal function.
36. Drug interactions
’ü¼ There are some drugs which potentiates the
actions of sulfonylureas i. e. increase
hypoglycemic activity. They are ŌĆō
* NSAIDs
* Alcohol
* Coumarin
* Antibacterial agents
* Antifungal agents
37. ’ü¼ Also there are some drugs which
antagonises the action of sulfonylureas i. e.
decrease hypoglycemic activity. They are ŌĆō
* Thiazide
* Frusemide
* Thyroid hormone
* Corticosteroids
* Oral contraceptives.
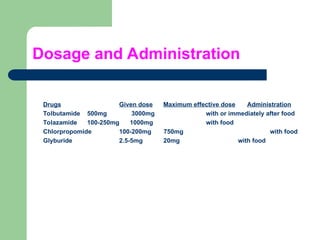
38. Dosage and Administration
Drugs Given dose Maximum effective dose Administration
Tolbutamide 500mg 3000mg with or immediately after food
Tolazamide 100-250mg 1000mg with food
Chlorpropomide 100-200mg 750mg with food
Glyburide 2.5-5mg 20mg with food
40. Mechanism of action
’ü¼ 1. Biguanides Directly stimulate glycolysis in
peripheral tissues with increased glucose
removal from blood.
’ü¼ 2. Reduce blood glucose level by reducing
hepatic gluco-neogenesis.
’ü¼ 3. Reduce intestinal glucose absorption.
’ü¼ 4. Enhancement of insulin receptor binding.
41. Pharmacokynetics
’ü¼ Route of administration : Oral.
’ü¼ Absorption : Small intestine.
’ü¼ Metabolism : Does not bound to plasma
protein.
’ü¼ Excretion : Excreted unchanged in urine.
’ü¼ Plasma half life : About 2 hours.
45. Drug interaction
’ü¼ With insulin, does not show any action.
’ü¼ With sulfonylureas, show effective action
when a single drug has proved to be
ineffective.
’ü¼ Cimetidine increases the absorption of
Metformin and decreases the renal
clearance.