














































![abour_and_partogram[1].pptxbshshdhdhshsj](https://cdn.slidesharecdn.com/ss_thumbnails/stagesoflabourandpartogram1-241026060027-dd0786c1-thumbnail.jpg?width=560&fit=bounds)



More Related Content
Similar to SECOND STAGE-OF LABOUR.pptx (20)
Recently uploaded (20)













SECOND STAGE-OF LABOUR.pptx
- 1. SECOND STAGE
- 2. INTRA PARTUM MONITORING The nature of the transition and Second stage Phase of labour The second stage of labour has traditionally been regarded as the phase between full dilatation of the cervical os and the birth of the baby. UTERINE ACTION Contraction become stronger and longer allowing both mother and fetus regular recovery periods. The membrance often rupture spontenously towards the end of the first stage. The conequent drainage of liqur allows the hard round fetal head to be directly applied to the verginal tissues.
- 3. This pressure aids distortions. Fetal arial pressure increase thereon of the head, resulting in smaller pressuring diameters more radial proress and less trauma to both mother and fetus. The contractions become expulsive as the fetus descends further into the vagina. Pressure from the presenting part stimulates nerve receptor in the pelvic floor. This phenomenon Is termed the Ferguson refute.
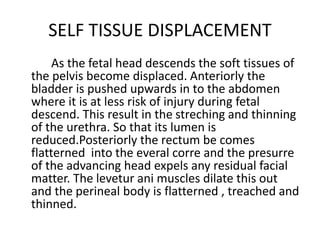
- 4. SELF TISSUE DISPLACEMENT As the fetal head descends the soft tissues of the pelvis become displaced. Anteriorly the bladder is pushed upwards in to the abdomen where it is at less risk of injury during fetal descend. This result in the streching and thinning of the urethra. So that its lumen is reduced.Posteriorly the rectum be comes flatterned into the everal corre and the presurre of the advancing head expels any residual facial matter. The levetur ani muscles dilate this out and the perineal body is flatterned , treached and thinned.
- 5. Tontraction and the fetal head becomes viible at ultra advancing with each contraction and recoding between contraction unit crowning takes place. The follow with the next contraction accompanied by a gush of aminotic fluid and sometimes of blood. The econd stage culmintaes in the birth of the baby.
- 6. RECOGNITION OF THE COMMENCEMENT OF THE SECONFD STAGE OF LABOUR Progress from the first to the second stage is not always clinically apparent.
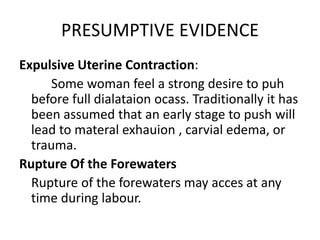
- 7. PRESUMPTIVE EVIDENCE Expulsive Uterine Contraction: Some woman feel a strong desire to puh before full dialataion ocass. Traditionally it has been assumed that an early stage to push will lead to materal exhauion , carvial edema, or trauma. Rupture Of the Forewaters Rupture of the forewaters may acces at any time during labour.
- 8. Dialatation and Gapping of the anes: Deep engagement of the presenting part may produce this during during the latest phase of the first stage. Analcleftline Some midwives here reported observing this line a a pigment make in the cleff of the button which crops upto the anal cleft as the labour progress also called as people line.
- 9. Appearances of the rhomboid of michaclis This is sometime noted when a women is in position where her back is visible .It present as a dove shaped crove in the lower back and is held to indicate the posterior displacement rof the moras into the maternal acrial curvr. This seems to labouring women to arch her back puh he buttocks forward and throw her armes back to grasp and fired object she can find.
- 10. Upper Abdominal Pressure and Epidrial Analysia It has been observed anecdotally that women who have an epideral instit often have a sense of discomfort under the ribs toward the end of the first stage of labor. SHOW This I the los of blood srtain nussess which often accompanies rapid dilation of the cervical as towards the end of the first stage of labor.
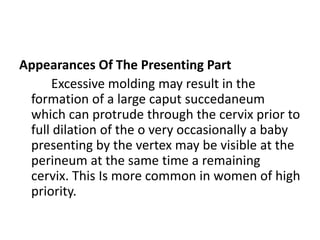
- 11. Appearances Of The Presenting Part Excessive molding may result in the formation of a large caput succedaneum which can protrude through the cervix prior to full dilation of the o very occasionally a baby presenting by the vertex may be visible at the perineum at the same time a remaining cervix. This Is more common in women of high priority.
- 12. Confirmatory Evidence: In many midwifery settings it Is held that regional examination must be undertaken to confirm full dilation of the cervical os. This Is both to ensure a women is not puhing too early and to provide a base line. For timing the length of the second stage of labor
- 13. PHASE AND DURATIONS The Latent Phase In some woman full dilation of cervical as is recorded but the presenting part may not yet have reached the pelvic outlet. She may not experience a strong expulsive urge until the head has descended sufficiently to even pressure on the return and perinea tissues.
- 14. Active Phase Once the fetal head Is visible the women will usually experience a compulsive urge to puh. Duration of the Second Stage There is no good evidence about the absolute time limit of physiological labor. It average 2hrs in primigavide and 30 mits in multiphase.
- 15. The Mechanisam of Normal Labor As the fetus descends soft tissues and body structures exact preserves which lead to decent through the birth canal by a cervices movements. Collectively three movements one called the mechanism of labour
- 16. PRINCIPLE COMMON TO ALL MECHANISMS ARE ÔÉò Decent takes place. ÔÉò Whatever part leads and first meets the resistance of the pelvic flar will rotate towards until it comes under the symphyics parts ÔÉò Whatever emerges from the pelvic will pivot around the pubic bone. ÔÉò The live is longitudinal ÔÉò The presentation is cephalic ÔÉò The position to right or left ocipi to anterior ÔÉò The attitude I one of the good florion ÔÉò The Denomination is the aciput ÔÉò The presenting part is the posterior part of the anterior partal bone.
- 17. MAIN MOVEMENT OF THE FETUS Descent Decent of the fetal head into the pelvic often begins before the arrest of the labor. For a primigravid woman this usually occurs during the later weeks of preganancy. In multigravid woman muscle tone is often more lax and therefore descent and engagement of the fetal head may not occur until labor actually begins . Through out the first stage of labor the contraction and retraction of the where muscles allow lers room in the utrus exerting pressure on the fetus to descend further. Following rupture of the jore water and the exertion of material effort, progress speeds up.
- 18. FLXION This increase throughout the labor . The fetal spine is attached nearest the posterior part of the skull, pressure exerted down the fetal arias will be more forcibly transmize to the output than the siniput. The effect Is to increase theron when results in smaller presnting diameter which will negotiate the pelvi more easily. At the outset of labour the suboccipilo fontal diamate , which Is on average approximately 10 cm is presenting with greater function the ubocipho pregmativ diameter on average approximately 9. cm pesents. The output becomes the leading part.
- 19. Internal Rotation Of the Head Duing a contruction the leading part is pushed onwards onto the pelvic floor. The resistance of thi muscular diaphrighn bring about rotation . As the construction fades the pelvic floor rebounds caring the output to glid towards resistance Is therefore as important determinant of rotation . This explains why the rotations is often delayed following epidunal analyia which cover relatiob of pelvic floor muscle. The selope of the pelvic floor determines the dimention of rotation
- 20. The muscles are hammer shaped and slope down anteriorly , so whichever part of the fetu first meets the laternal half of this slope will be directed forwards and towards the center. In a well flex restore presentation the output lead and rotate extremely through 1/8 of a circle when it meets the pelvic floor. This causes a slight twist in the neck as head is no longer in direct alignment with the shoulders. The anteroposterior diameter of the head now lies in the wildest diameter on the pelvic outlet. The ouput lips beneath the sub public arch and crowling awr when the head no longer recedes between contraction and the widest maniverse diameter is born. If fetu I maintained the subacipitobromatic diameter uually approximately 9.cm distrens the vaginal arifire.
- 21. EXTENSION OF THE HEAD Once crowning has occurred the fetal head can extend piroting on the subaciptal region around the pelvic bone. This releases the sinipet face and chin which sweep the perinium and then are born by a movement of extenion
- 22. RESTITUTION The twist in the neck of the fetus which resulted from internal rotation Is not connected by a slight untwisting movemet. The output mores I of a circle toward the side from which I shatered
- 23. INTERNAL ROTATION OF THE SHOULDERS The shoulders undergo a similar rotation to that of the head to lie in the widest diameter of the pelvic outlet namely enteroposteries. The anterior shoulder is the first to reach the elevator ani muscle and it therfore rotates anteriorly to live under the symphysis pubies. Thus movement can be clearly seen as the head turns at the same time. It occurs in the same direction as restitution and the accept of the fetal head now lies laterally.
- 24. LATERAL FLEXION The shoulder are usually born sequentially . When the mother Is in a supported sitting positions, the anterior shoulder is usually born first. Although it has been noted by midwives who commonly use upright or kneeling positions that the posterior shoulder is commonly seen first. In the former care the anterior shoulder lips beneath the sub public arch and the posterior shoulder posses over the perinum. This enables a smaller diameter to distend the vaginal orifice. Then if both shoulder were born simultaneously. The remainder of the body Is born by lateral flexion a the spine bends sideways through the curved birtgcanel