






































Serial extraction
- 2. ï History ï Concept ï Rationale ï Indications ï Contraindications ï Methods ï Special situations ï Advantages ï Disadvantages ï Conclusion
- 3. ï âMalocclusion of teeth frequently constitutes an indignity with profound mental and physical stigma on our child patients. Their well being is our challenging obligation.ââ
- 4. ï Introduced the concept of Serial Extraction ï Coined the term âSerial Extractionâ
- 5. ï The term serial extraction describes an orthodontic treatment procedure that involves the orderly removal of selected deciduous and permanent teeth in a predetermined sequence
- 6. ï Nance popularized this technique and termed it âplanned & progressive extractionâ. ï Hotz in 1970 called âactive supervisionâ of teeth by extraction.
- 7. ï Anticipate ï Minimize deformity ï Records and analysis
- 9. ï Selection of cases ï Ideal timing â First permanent anterior tooth erupts. ï X-rays ï Horizontal growth ï Time to align
- 10. ï If distance of half or more premolar is lacking in both sides of the lower arch
- 11. ï From C â More than compensated by Canine ï From D â ï From E â Mesial drift of FPM
- 12. ï Arch Length tooth material discrepancy ï Physiologic tooth movement
- 13. ï Class 1 malocclusion with > 10 mm discrepancy ï No developmental spacing ï Aberrant eruption pattern ï Crowding with proclination ï Lingual eruption of lateral incisor
- 15. ï Midline shift due to lateral incisor displacement ï Labial displacemnet of mandibular incisors ï Gingival recession of labially placed incisors ï Premature loss of primary canine ï Labially placed but unerupted permanent canine
- 16. ï Congenital absence of teeth ï Cleft lip palate patients ï Midline diastema ï Vertical discrepancy: deep bite or open bite
- 17. ï Class 1 malocclusion with minimal discrepancy ï Class ll div ll ï Class lll ï Skeletal class lll ï Collapsed arch
- 18. ï 80% of class 1 crowded arches are not self correcting. ï 3rd molar impaction if lower incisors are crowded ï Greater the discrepancy between tooth size and basal boneâĶ better is the prognosis of SE
- 19. ï Earlier the extraction of the primary teeth better is chance of self correction of rotation. Except ï Not very severe crowding and lower incisors are lingually inclined. Deep bite.
- 20. ï Dewelâs method ï Tweedâs method ï Nanceâs method ï Moyerâs method
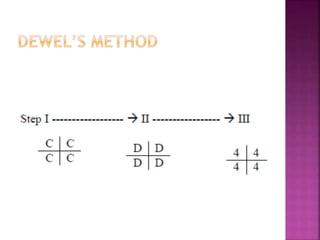
- 23. ï First: Deciduous canines: to permit eruption and optimal alignment of lateral incisors. ï Second: First deciduous molars: to accelerate eruption of first premolars ahead of canine if possible. ï Third: Erupting first premolars: Before the first premolars are extracted, all the diagnostic criteria must again be evaluated.
- 24. 7 Â― to 8 Â― years ï First: Around 8 years all âDâ. Maintain âCâ to retard eruption of permanent canines. ï Second: Extraction of â4â and âCâ should be done 4-6 months prior to eruption of permanent canines when they erupt they migrate posteriorly into good position.
- 27. ï Similar to the Tweedâs technique ï âDâ extracted before 6 â 12 m of its normal exfoliation time 1st Premolars & the deciduous canines.
- 28. When crowding is in central incisor region. After eruption of lateral incisors. ï Stage I - B central incisors. ï Stage II - C after 7-8m lateral incisors ï Stage III â D Stimulates eruption of all first premolars. ï Stage IV â 4 after 7-8m space for and stimulation of eruption of canines.
- 31. ï Earlier the extraction better the self correction of rotation. BUT ï If lowers are lingually inclined do not extract early.
- 32. ï Premature removal is not indicated ï Remove when Â― - 2/3 of root is formed ï Remove when canines have erupted first ï Extract erupting PM as early as possible Time for posteriors to drift.
- 33. Any remaining primary incisor can be extracted
- 34. ï In borderline cases 2nd PM can be extracted ï If position of canine is very abnormal it can be extracted instead of PM ï If 2nd PM or 1st permanent molar have large fillings they should be extracted in preference to 1st PM ï Permanent first Molar!
- 35. ï Less need of retention ï Less severe malocclusion ï Physiological tooth movement
- 36. ï Deepening of overbite (Dewel 1967) ï Rotation of teeth ï Failure of complete space closure ï Lingual collapse of mandibular arch ï Patient cooperation and long follow up
- 38. (1) Developing dentition receives competent supervision (2) no teeth of any kind be removed prior to a most precise and exacting case analysis (3) case analysis be repeated preceding and subsequent extraction (4) that when indicated, competent orthodontic treatment be provided
- 39. ï Kjellgren, B. Serial extraction as a corrective procedure in dental orthopedic therapy. Trans. Europ. Orthod. Soc. 1947â 1948;:134â160. ï Hotz, R. Active supervision of the eruption of teeth by extraction. Trans. Europ. Orthod. Soc. 1947â1948;:34â47.i ï Manual of Pediatric dentistry; Sridhar Premkumar ï Orthodontics âThe art and scienceâ Dr. B.S.Iyyer.
- 42. Q1. Early extraction of primary first molar can cause a. Early eruption of permanent first molars b. An Increase in overjet c. Abnormal swallowing pattern d. Worsening of deep bite
- 43. Q2. Disadvantage of serial extraction is a. Supra eruption of antagonist tooth b. Rotation of teeth c. Increase in open bite d. Greater need of retention following treatment
- 44. Q3. The term âserial extractionâ was coined by a. Heath (1961) b. Robert Bunon (1743) c. Kjellgren (1929) d. Dewel (1969)
- 45. Q4. In a case of moderate to severe crowding permanent canine can be extracted when a. Inspite of serial extraction there is tooth material excess b. When the permanent canine is severly malposed c. Skeletal Class lll with mandibular excess
- 46. Q5. Early extraction of primary first molar can cause a. Early eruption of permanent first molars b. An Increase in overjet c. Abnormal swallowing pattern d. Worsening of deep bite