



















































SPN-Imaging of Solitary Pulmonary Nodules.pptx
- 1. Imaging Evaluation of Solitary Pulmonary Nodules Presenter ŌĆō Suleyman Fantahun, Y-I Radiology Resident Moderator ŌĆō Abdi Alemayehu, MD, Assistant Professor of Radiology
- 2. Outline ŌĆó Definition ŌĆó Significant of SPN in imaging ŌĆó Imaging modalities ŌĆó Morphologic features ŌĆó Decision analysis ŌĆó Reference 4/6/2024 2
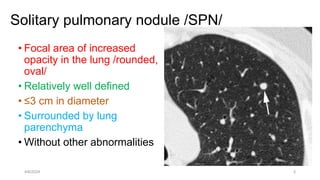
- 3. Solitary pulmonary nodule /SPN/ ŌĆó Focal area of increased opacity in the lung /rounded, oval/ ŌĆó Relatively well defined ŌĆó Ōēż3 cm in diameter ŌĆó Surrounded by lung parenchyma ŌĆó Without other abnormalities 4/6/2024 3
- 4. Significance of SPN ŌĆó How Common are they? ŌĆó 25% of healthy adult volunteers and 51% in lung cancer screening population ŌĆó Why bother studying them? ŌĆó SPN may be early lung cancer (mortality rate = 85%) ŌĆó 20-30% present as SPN. ŌĆó Early detection of small nodules reduce lung cancerŌĆōspecific mortality 4/6/2024 4
- 6. Goal of imaging ŌĆó Establishing a diagnosis based solely on the imaging features is usually not possible. but, ŌĆó Radiographic features are important to determine the likelihood of malignancy. ŌĆó Eventually commencing Noninvasive imaging-based assessment and management of SPNs 4/6/2024 6
- 7. Imaging modalities ŌĆó Radiograph ŌĆō new: ŌĆó Fluoroscopy ŌĆó CT ŌĆó PET ŌĆó PET-CT ŌĆó Image guided Biopsy 4/6/2024 7
- 8. Clinical Evaluation ŌĆó Independent predictors of malignancy ŌĆó Advanced age ŌĆó Current or past smoking habit ŌĆó History of extra-thoracic cancer more than 5 years before detection of a nodule 4/6/2024 8
- 9. ContŌĆ” ŌĆó An SPN (likelihood of metastasis) ŌĆó In the absence of a known prior malignancy ŌĆó Unlikely to be a metastasis ŌĆó With melanoma, sarcoma, or testicular carcinoma ŌĆó Malignant SPN is 2.5x likely to be metastasis than a primary lung cancer ŌĆó With head and neck SCC ŌĆó Malignant SPN is 8x likely to be a primary lung cancer 4/6/2024 9
- 10. Imaging Evaluation ŌĆó Steps:- ŌĆó Is it really SPN? ŌĆó Classify:- ŌĆó Solid nodule ŌĆó Sub solid nodule /SSN/ ŌĆó Pure Ground Glass Attenuation Nodule /GGAN/ ŌĆó Partly Solid nodule /PSN/ ŌĆó Asses the likelihood of malignancy. 4/6/2024 10
- 11. Size ŌĆó How to measure? ŌĆó Smallest diameter?, largest?, average of both . ŌĆó For solid nodules: 4/6/2024 11
- 12. Margin and Contour ŌĆó Irregular, lobulated contour with spiculated margin. ŌĆó Malignant (90%) 4/6/2024 12 ŌĆó Smooth surface contour, sharply defined edge ŌĆó Malignant (20%) ŌĆó Metastases ŌĆó Carcinoid tumors
- 13. ŌĆó Pleural tail sign ŌĆó Thin linear opacity extending from the edge of a nodule to the pleural surface ŌĆó Represents Fibrosis 4/6/2024 13 ŌĆó Halo sign ŌĆó A halo of GGO surrounding a soft tissue density lung nodule ŌĆó Could represent ŌĆó Hemorrhage, lepidic spread of tumor
- 14. ŌĆó Reverse Halo sign (Atoll sign) ŌĆó Central area of GGO surrounded by a rim of consolidation, ŌĆó COP, Lung cancer after radiofrequency ablation 4/6/2024 14
- 15. ŌĆó Air bronchograms ŌĆó Commonly seen in malignant nodules(29%) than in Benign(6%) 4/6/2024 15 ŌĆó Pseudocavitation ŌĆó Small rounded lucencies, not representing air bronchograms or cavitation
- 16. 4/6/2024 16 ŌĆó Cavitation ŌĆó Wall thickness ŌĆó < 5 mm ŌĆó 92% benign ŌĆó 5 to 15 mm ŌĆó 49% malignant ŌĆó > 15 mm ŌĆó 95% malignant ŌĆó Benign lesions often have a thin, smooth wall ŌĆó Malignant lesions tend to have a thick, nodular wall
- 17. ŌĆó Air-fluid Level ŌĆó Indicate a benign lesion ŌĆó Bacterial lung abscess ŌĆó Uncommon in cavitary carcinoma, cavitary TB and fungal infections 4/6/2024 17 ŌĆó Satellite Nodules ŌĆó Small nodules seen adjacent to a larger nodule ŌĆó Predict a benign lesion ŌĆó Granulomatous diseases ŌĆó In Sarcoidosis ŌĆ£Galaxy signŌĆØ
- 18. 4/6/2024 18 Calcification - Benign Patterns
- 19. 4/6/2024 19 ŌĆó May be seen in benign SPNs but are visible in as many as 10% to 15% of cancers Indeterminate patterns
- 20. 4/6/2024 20
- 21. Fat ŌĆó CT ŌĆó (ŌłÆ40 to ŌłÆ120 HU) ŌĆó Most likely hamartoma lipoma, or lipoid pneumonia ŌĆó Presence in SPN is sufficient for calling it benign ŌĆó N.B: Follow-up is appropriate. 4/6/2024 21
- 22. Nodule Location ŌĆó About two thirds of lung cancers occur in the upper lobes ŌĆó Sixty percent of cancers ŌĆó Lung periphery ŌĆó Metastatic tumor ŌĆó Subpleural or outer third of the lung ŌĆó 2/3rd in the lower lobes ŌĆó TB ŌĆó Apical or posterior upper lobes, superior segment of the lower lobes 4/6/2024 22
- 23. Nodule Enhancement ŌĆó CT enhancement ŌĆó Only in spherical nodules with homogeneous attenuation ŌĆó Malignant nodules ŌĆó > 20 HU ŌĆó Benign nodules ŌĆó < 15 HU 4/6/2024 23
- 24. 4/6/2024 24
- 25. Nodule Growth ŌĆó Nodules are usually spherical, nodule volume = 4ŽĆr3 ŌĆó Assessed by volume doubling time ŌĆó Manifests as a 26% increase in diameter ŌĆó Limitations ŌĆó Small nodules ŌĆó Change in diameter is difficult to perceive ŌĆó Subsolid nodules ŌĆó Small and poorly defined, growth is difficult to perceive 4/6/2024 25
- 26. ContŌĆ” ŌĆó Solid SPN - Volume doubling time ŌĆó <20 days ŌĆó Infectious or inflammatory ŌĆó < 100 days /20ŌĆō400 days/ ŌĆó Malignant ŌĆó >400 days ŌĆó Benign ŌĆó Stable size over a 2-year period (>730 days) is benign. ŌĆó NEW* = 2-mm threshold for growth 4/6/2024 26
- 27. Unusual patterns of growth ŌĆó Temporary regression of SPNs 4/6/2024 27
- 28. ContŌĆ” ŌĆó Increased wall thickness 4/6/2024 28
- 29. Subsolid nodules /SSN/ ŌĆó Persistent subsolid nodules are more likely to be malignant. ŌĆó After an SSN is initially detected, reassessing with CT at 3 months. ŌĆó For persistent SSNs, CT features important for differentiating benign from malignant nodules: ŌĆó Nodule attenuation ŌĆó Presence and size of any solid component 4/6/2024 29
- 30. 4/6/2024 30
- 31. ContŌĆ” ŌĆó Solid component in SSN represents: ŌĆó Invasive component and/or ŌĆó Fibrosis with alveolar collapse ŌĆó To characterization of the degree of invasion in SSN: ŌĆó Mean nodule attenuation number ŌĆó Ratio of the solid-to-ground glass attenuation portions 4/6/2024 31
- 32. ŌĆó Ratio of the solid-to-ground glass attenuation portions ŌĆó Ōēż50% ŌĆó Air-containing type, Most are Adenocarcinoma in situ ŌĆó >50% ŌĆó Solid type, most are invasive adenocarcinoma 4/6/2024 32
- 33. Growth in SSN ŌĆó Sub solid Nodules ŌĆó Volume doubling of GGAN > PSN > Solid lesions ŌĆó Growth may manifest as: 1. Increase in size, 2. Increase in attenuation, 3. Development of a solid component 4. Increase in size of a solid component. ŌĆó Another method ŌĆō Mass of nodule (volume x density) 4/6/2024 33
- 34. 4/6/2024 34
- 35. 4/6/2024 35
- 36. 4/6/2024 36
- 37. Nodule Metabolism ŌĆó FDG-PET ŌĆó High sensitivity and specificity in Solid nodules Ōēź 10 mm ŌĆó Standardized uptake value (SUV) ŌĆó Benign Vs Malignant nodules ŌĆó SUV cutoff of 2.5 ŌĆó Visual analysis is as accurate ŌĆó PET/CT ŌĆó Be careful of Artifacts and misregistration 4/6/2024 37
- 38. 4/6/2024 38
- 39. Decision Analysis: Management ŌĆó For nodules that are detected incidentally ŌĆó The Fleischner Society Guideline ŌĆó American College of Chest Physicians (ACCP) ŌĆó Screening-detected Nodules ŌĆó LUNG-RADS (Lung Imaging Reporting and Data System) by ACR 4/6/2024 39
- 40. 4/6/2024 40
- 41. 4/6/2024v 41
- 42. Updated Fleischner Society Guidelines for Managing Incidental Pulmonary Nodules ŌĆó Population(s) not intended ŌĆó Ōēż 35 years ŌĆó Patients with Known Malignancy ŌĆó Immunocompromised Patients ŌĆó Lung Cancer Screening Population ŌĆó Slice selection ŌĆō 1.0 - 1.5mm thin ŌĆó Nodule in thick(>2mm) sections ŌĆó Follow up thin section, if size >6mm 4/6/2024 42
- 43. Risk Factors ŌĆó Older age ŌĆó Heavy smoking, ŌĆó Larger nodule size, ŌĆó Upper lobe location, and/or ŌĆó Nodule margin irregularity or spiculation Risk Categories ŌĆó Low ŌĆó <5% risk of cancer ŌĆó Intermediate ŌĆó 5%ŌĆō65% risk ŌĆó High ŌĆó >65% estimated risk 4/6/2024 43
- 44. Scenarios ŌĆó Single solid 6ŌĆō8-mm nodules in low-risk patients ŌĆó Well-defined with benign appearance at 12ŌĆō18 months ŌĆó Discontinue follow up ŌĆó GGNs smaller than 6 mm ŌĆó Suspicious features such as spiculation and fissure distortion ŌĆó Follow-up examination at 2 years the 4 years. 4/6/2024 44
- 45. 4/6/2024 45
- 46. ContŌĆ” ŌĆó A decrease in size accompanied by an increase in density ŌĆó Warrants imaging surveillance ŌĆó Peri-fissural nodule ŌĆó Triangular or lentiform morphology, smooth contours, and sharp margins ŌĆó Benign Intrapulmonary lymph nodes ŌĆó No follow-up CT ŌĆó Suspicious features ŌĆó Follow up CT 4/6/2024 46
- 47. ŌĆó Suspicious features: contour spiculation (a), fissural transgression (b), fissural distortion (arrow) (c), and a juxtafissural nodule not entirely associated with the fissure (d). 4/6/2024 47
- 48. 4/6/2024 48
- 49. ŌĆó Cystic lung lesion - could occur by: ŌĆó Cystification of a nodule ŌĆó Tumor arising from the wall of a preexisting cyst ŌĆó Suspicious features: ŌĆó Asymmetric wall thickening ’ā© endophytic or exophytic mural nodule 4/6/2024 49
- 50. 4/6/2024 50
- 51. 4/6/2024 51
- 52. 4/6/2024 52
- 53. 4/6/2024 53
- 54. References 1. THORACIC IMAGING Pulmonary and Cardiovascular Radiology, Third Edition, (Page 952-1004) 2. Update in the Evaluation of the Solitary Pulmonary Nodule, RSNA, 2014 3. The Solitary Pulmonary Nodule - The NEJM, 2003 4. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017 5. Solitary Pulmonary Nodules. Morphologic Evaluation ŌĆō RSNA, 2000 6. Updated Fleischner Society Guidelines for Managing Incidental Pulmonary Nodules: Common Questions and Challenging Scenarios, RSNA, 2018 4/6/2024 54
- 55. Thank You.
Editor's Notes
- #4: SPN is a discrete, well-marginated, rounded opacity less than or equal to 3 cm in diameter that is completely surrounded by lung parenchyma, does not touch the hilum or mediastinum, and is not associated with adenopathy, atelectasis, or pleural effusion.
- #12: The smaller the nodule the more likely it is benign.
- #13: Adenocarcinoma Hamartoma Metastasis from head and neck SCC
- #14: Adenocarcinoma. HRCT shows an irregular, spiculated nodule with multiple pleural tails. Air bronchograms are visible within the nodule Halo sign in invasive aspergillosis Halo sign in adenocarcinoma. HRCT shows a dense central nodule surrounded by a halo (arrows). In adenocarcinoma, the dense center usually represents invasive growth, while the halo represents the presence of lepidic tumor growth.
- #15: Figure 2. Reverse halo sign after radiofrequency ablation of a pulmonary metastasis in a 63-year-old man with pancreatic cancer who previously underwent left upper lobectomy. (a) Contrast-enhanced CT image shows a left-lower-lobe metastasis (arrow). (b) Contrastenhanced CT image obtained 1 month after radiofrequency ablation shows the treated metastasis (arrow), which now has mixed attenuation, surrounded by a ground-glass opacity (*) and a well-circumscribed rim of consolidation (arrowheads), a finding known as the reverse halo sign. Originally described in cryptogenic organizing pneumonia, the reverse halo, or atoll, sign can also be seen in paracoccidioidomycosis, tuberculosis, lymphomatoid granulomatosis, Wegener granulomatosis, sarcoidosis, and tumors after radiofrequency ablation
- #16: 1. Adenocarcinoma. HRCT shows an irregular, spiculated nodule with multiple pleural tails. Air bronchograms are visible within the nodule. 2. Adenocarcinoma with a spiculated margin seen on CT. Two pleural tails (arrows) extend to the pleural surface. This appearance has been termed corona radiata or corona maligna. The surface of the nodule is lobulated and shows notches, both of which are findings indicating malignancy. Several lucencies within the nodule represent air bronchograms of areas of pseudocavitation, typical findings in adenocarcinoma and BAC.
- #17: Thin-walled lung cavities. A: In a patient with a persisting lung cavity from Coccidioides immitis infection, the wall is thin and smooth, measuring less than 5 mm in thickness. Cavitary adenocarcinoma shown on HRCT in six contiguous scans. The nodule contains an irregular cavity; is irregular and lobulated in shape, notched, and spiculated; and is associated with pleural tails. It also contains several air bronchograms.
- #18: Cavitary squamous cell carcinoma shown at two levels. The wall of the cavity is irregular, with several thick nodular regions (white arrow). The cavity contains an air-fluid level (black arrows). This is uncommon in malignancy and may represent hemorrhage or infection. 1. Tuberculosis. A right upper lobe nodule is associated with satellites (arrows). This appearance is most typical of a benign process but sometimes is seen with carcinoma.
- #19: Homogeneous calcification. Dense and uniform calcification (B) of a small right upper lobe nodule (arrow, A) is typical of a benign lesion, usually a tuberculoma. Dense central or ŌĆ£bullŌĆÖs-eyeŌĆØ calcification in a hamartoma. A round lung nodule (arrows) adjacent to the descending aorta shows dense central calcification. This is typical of histoplasmoma or hamartoma. Concentric or ŌĆ£targetŌĆØ calcification (arrow). One or more rings of calcium may be seen. This pattern is typical of a histoplasmoma. Multiple confluent nodular foci of calcification (ŌĆ£popcornŌĆØ calcification; arrow) in a hamartoma. This appearance is typical of hamartoma and corresponds to the calcification of cartilage nodules.
- #20: Eccentric calcification in an adenocarcinoma. A lobulated mass shows a small focus of eccentric calcification (arrow).
- #21: Carcinoid tumor with stippled calcifications. A: A sharply marginated lung mass is visible. B: CT shows a sharply marginated, lobulated mass with multiple small foci of calcification.
- #22: Figure 3. Hamartoma in a 72-year-old woman with an unknown primary malignancy that metastasized to the liver. Contrast-enhanced CT image shows a well-circumscribed left-lower-lobe nodule (arrow) with low attenuation (-46 HU), a finding consistent with fat. Focal fat can also be seen in a pulmonary nodule in liposarcoma metastases and lipoid pneumonia.
- #25: CT enhancement study in a 54-year-old woman with endometrial hyperplasia. CT images obtained before (a) and after (b) administration of intravenous contrast material show the nodule has enhanced, with an increase in attenuation values of 109 HU. Typically, malignant nodules enhance with an increase in attenuation values of more than 20 HU, whereas benign nodules enhance with an increase in attenuation values of less than 15 HU. Results from transthoracic needle aspiration biopsy revealed carcinoid tumor
- #28: Transient decrease in size of a lung cancer. (a) CT image obtained at the patientŌĆÖs initial presentation shows a nodule (arrow) in the left lower lobe. (b) Follow-up CT image obtained 1 year later shows the nodule (arrow), which decreased in size. (c) CT image obtained 2 years after the initial presentation shows the nodule (arrow), which increased in size and lobularity. Although most lung cancers grow at a steady rate, temporary regression and growth can occur. It is postulated that a transient decrease in size may be related to the development of a fibrous component and/or collapse of fibrosis. Accordingly, a decrease in size requires continued imaging reassessment to confirm long-term stability or resolution.
- #29: Lung cancer manifesting with increased wall thickness of a cystic airspace in a 77-year-old man with a history of right upper lobectomy for adenocarcinoma. (a) Contrast-enhanced CT image shows a cystic airspace (*) in the right lower lobe. (b) Follow-up CT image obtained 6 months later shows a new soft-tissue component (arrows) along the wall of the cystic airspace. Results of histologic analysis of the soft-tissue component revealed adenocarcinoma. The finding of an isolated cystic airspace with increased wall thickness should raise the suspicion for lung cancer
- #31: Figure 7. IASLC, ATS, and ERS classification of lung adenocarcinoma, in which preinvasive lesions include atypical adenomatous hyperplasia (AAH) and adenocarcinoma in situ (AIS), both of which are defined as lesions with purely lepidic growth along the alveolar surface. (a) CT image shows an AAH lesion (arrow), which typically has pure ground-glass attenuation and measures less than 1 cm. However, lesions larger than 1 cm have been reported. (b) CT image shows an AIS lesion (arrowheads), which typically has pure groundglass attenuation and measures less than 3 cm. Invasive lesions include minimally invasive adenocarcinoma (MIA) and invasive adenocarcinoma, which are further classified as having a lepidic, acinar, papillary, micropapillary, or solid-predominant pattern. (c) CT image shows an MIA lesion (arrow), which has a predominantly lepidic pattern; lacks necrosis; does not invade lymphatics, blood vessels, or pleura; measures less than 3 cm; and has an invasive component (arrowhead) that measures no more than 5 mm in any one location. (d) CT image shows a lepidic-predominant adenocarcinoma (LPA) in its nonmucinous form. Necrosis may be present, and the focus of invasion of lymphatics and blood vessels is greater than 5 mm.
- #33: Fleischner Society recommendations for measuring subsolid lesions at CT. (a) CT image obtained with narrow and/or mediastinal window settings shows the solid component (*) of a subsolid lesion. (b) CT image obtained with wide and/or lung window settings shows the ground-glass-attenuation component (arrowheads) of the lesion. Measurements are based on the average of the long and short axis dimensions. Determination of the percentage of solid to ground-glass-attenuation components is important, because the greater the solid component, the more likely that the lesion is an invasive adenocarcinoma. * = solid component
- #35: Subsolid lesion that increased in size, which indicates an increased risk for malignancy, in a 55-year-old man. (a) Coned-down contrast-enhanced CT image shows a 1.3-cm nodule (arrow) with pure ground-glass attenuation in the left lower lobe. Pulmonary vessels are visible within the lesion. The Fleischner Society recommends that solitary pure GGANs larger than 5 mm undergo initial follow-up CT in 3 months to determine persistence followed by yearly surveillance CT for a minimum of 3 years if the nodule is persistent and remains unchanged. This lesion persisted at 3-month follow-up CT. (b) Follow-up CT image obtained 3 years later shows the lesion, which increased in size to 1.8 cm. Biopsy was performed, and results of histologic analysis revealed adenocarcinoma. Because the volume-doubling time of subsolid lung cancers is typically longer than that for lung cancers that manifest as a solid nodule, imaging reassessment is recommended for an extended period of time for patients with a subsolid nodule.
- #36: (11) Increased attenuation in a subsolid lesion, which indicates an increased risk for malignancy. (a) Coned-down CT image of the chest with coronal reformation shows a 1.2-cm subsolid nodule (arrow) in the left upper lobe. (b) Follow-up CT image obtained 1 year later shows the nodule (arrow), which demonstrates increased attenuation, in addition to an increase in the overall size. According to the American College of Chest Physicians (ACCP) algorithm, an increase in nodule attenuation should be interpreted as an indicator of possible malignancy, and, in most cases, surgical resection should be strongly considered.
- #37: (12) Development of a soft-tissue component in a subsolid lesion, which indicates an increased risk for malignancy, in an 85-year-old man with a history of adenocarcinoma that was treated with right upper lobectomy. (a) Contrast-enhanced CT image shows a 1.8-cm nodule with pure ground-glass attenuation (arrow) in the left upper lobe. Pulmonary vessels and the air bronchogram sign are visible in the lesion. (b) Follow-up CT image obtained 3 months later shows the nodule (arrow), with a new solid component posteriorly (arrowhead). Biopsy was performed, and results of histologic analysis revealed adenocarcinoma. A direct correlation between the soft-tissue component and the degree of invasion or aggressiveness of subsolid adenocarcinomas and patient prognosis and survival has been reported
- #38: Alternative to measuring nodule enhancement in the evaluation of solid SPNs. FDG is a measure of glucose metabolism
- #39: Figure 18. Infection mimicking malignancy in a 30- year-old man with no symptoms and a right lower lobe mass detected at chest radiography performed for a routine occupational health examination. (a, b) Unenhanced CT (a) and PET/CT (b) images show a 3-cm solid lesion in the right lower lobe (arrow in a) with a maximum SUV of 16.7. Biopsy results revealed granulomatous inflammation and no malignant cells. (c) Followup CT image obtained 2 months later shows regression of the lesion (arrow). Infectious and inflammatory conditions can accumulate FDG and be misinterpreted as malignant. Figure 16. PET-negative neuroendocrine tumor in a 59-year-old woman. Unenhanced CT (a) and PET/CT (b) images show a well-circumscribed nodule in the middle lobe (arrow) with no FDG uptake. Results from transthoracic needle biopsy revealed a well-differentiated neuroendocrine tumor (carcinoid). False-negative PET findings can also occur in patients with indolent adenocarcinomas
- #46: Figure 2. GGN smaller than 6 mm. (a) Axial contrast materialŌĆōenhanced chest CT image (lung window) of the left lung shows a pure GGN in the lingula. There is retraction of the fissure (arrow), although it is subtle. Fissure retraction is a suspicious feature that warrants follow-up. (b) Axial nonenhanced chest CT image (lung window) obtained at 2-year follow-up shows an interval increase in the density of the nodule, with a new small solid perifissural component and progressive retraction of the fissure (arrow). These features are suspicious for malignancy
- #49: Figures 6, 7. (6) Perifissural nodule with suspicious features that warrant follow-up. (a) Axial nonenhanced chest CT image (lung window) of the right lung shows a 5-mm solid nodule (arrow) in the right middle lobe. The nodule has irregular contours and a juxtafissural location. (b) Axial nonenhanced chest CT image (lung window) obtained at 12-month follow-up shows interval growth of the nodule (arrow), with persistent contour irregularity. The lesion was found to represent a small invasive adenocarcinoma at resection
- #50: (10) Illustrations depict the suspicious features of cystic lesions: endophytic nodule (a), exophytic nodule (b), and asymmetric wall thickening (c).
- #51: Figures 9, 10. (9) Cystic lung lesion with suspicious features. (a) Axial contrast-enhanced CT image (lung window) of the right lung shows a cystic lesion in the right lower lobe. There is asymmetric wall thickening and an endophytic mural nodule (arrow), features that are highly suspicious for malignancy. (b) Sagittal contrast-enhanced CT image (lung window) better shows the endophytic nodule (arrow) in the inferior wall of the suspicious right lower lobe cystic lesion.