Spontaneous consecutive exotropia, 2022.pdf
ŌĆó
0 likesŌĆó26 views

Spontaneous consecutive exotropia was presented at the 5th Asean Ophthalmology Congress held online in 2022


Spontaneous consecutive exotropia, 2022.pdf
- 1. Spontaneous Consecutive Exotropia Alvina Pauline Santiago, MD
- 2. Case 1: 3, Male Sc MET 4PD, 30PD LE(T)ŌĆÖ Atropine +2.50 OU With +2.50, small MXT noted Given Plano A +1.50 cc 0-2 PD MET, ortho at near
- 3. Case 1: 3, Male Managed with reduced plus with Adds till age 7 Short-acting cycloplegia: +2.00 OU Given +1.00 OU
- 4. Case 1: 3 now 9 Lost to follow-up for 2 years Wearing a +1.00 prescribed from 2 years prior 30PD X(T) Subjective Refraction ŌĆóOD: -0.50 20/20 ŌĆóOS: -0.75 20/40 Cyclorefraction: +0.50, OU ŌĆóConservative management ŌĆóMyopic Rx ŌĆóConvergence exercises ŌĆóPatching
- 5. Case 1: 3 now 17 Findings ŌĆó -1.00 OU ŌĆó Orthotropia w correction ŌĆó 14PD X(T) without Rx
- 6. Case 1: 3 now 17 Findings ŌĆó -1.00 OU ŌĆó Orthotropia w correction ŌĆó 14PD X(T) without Rx Risk Factors ŌĆó Amblyopia ŌĆó Control of ET in 2 months ŌĆó IOOA ŌĆó Remote NPC ŌĆó High AC/A ŌĆó Lost to follow-up 2 years
- 7. Case 2: 9 mo, Male ŌĆó +3.00 OU, still w 30PD ET ŌĆó 40PD sc ŌĆó Atropine: +4.25 OU ŌĆó Age 1: Cycloplegic: +2.50 OU ŌĆó Reduced plus +1.50 OU controlled
- 8. Case 2: 9 mos, now 5 ŌĆóCyclorefraction: +2.00 OU ŌĆóReduced plus: ŌĆó+1.00 20/40 ŌĆó+1.00 20/60
- 9. Case 2: 9mo, now 7 ŌĆó Lost to follow-up for 2 years ŌĆó Wearing last known Rx +1.00 ŌĆó Monofixation Exotropia w/sc ŌĆó Cycloplegic refraction: +1.00 OU ŌĆó Patching ŌĆó Overminus lenses: -0.50 OU ŌĆó VA at least 20/40
- 10. Case 2: 9mo, now 9 Current Management ŌĆó Tolerated overminus: -1.00 OU ŌĆó 20/30 OU ŌĆó X(T) = 14PD ŌĆó Cycloplegic: plano OU ŌĆó -1.50: 12PD X(T) Risk Factors ŌĆó Amblyopia ŌĆó DVD ŌĆó Remote NPC ŌĆó Wrong glasses ŌĆó Lost to follow-up 2 years
- 11. Case 3: 1, Male Clinical Features ŌĆó ET 35PD ŌĆó Right preferred ŌĆó Surgery advised ŌĆó Membrane prisms ŌĆó Cyclo: +1.50 OU Risk Factors ŌĆó V pattern; IOOA ŌĆó DVD
- 12. Case 3: 1 now 5 ŌĆó18-25PD X(T) ŌĆóControlled w -1.50 OU ŌĆóRemote NPC
- 13. Case 3: 1, now 12 ŌĆó 12-16PD X(T) ŌĆó Over minus lenses: 10-16 X(T) ŌĆó Orthoptics Risk Factors ŌĆó Remote NPC ŌĆó Amblyopia ŌĆó DVD ŌĆó IOOA, V pattern ŌĆó Preterm
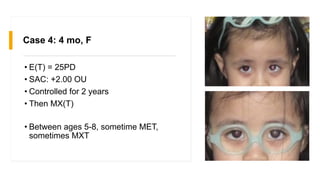
- 14. Case 4: 4 mo, F ŌĆó E(T) = 25PD ŌĆó SAC: +2.00 OU ŌĆó Controlled for 2 years ŌĆó Then MX(T) ŌĆó Between ages 5-8, sometime MET, sometimes MXT
- 15. Case 4: 4 mo, now 8 ŌĆó 20PD X(T) w DVD ŌĆó Best correction: ŌĆó OD: -0.25 20/25 ŌĆó OS: -1.00 -0.50 x 180 20/20 Risk Factors ŌĆó Variable monofixation? ŌĆó Amblyopia ŌĆó DVD ŌĆó E(T) recurrence
- 16. Take home message ŌĆó Spontaneous consecutive exotropia can occur: ŌĆó Accommodative esotropia ŌĆó Infantile esotropia (managed with prisms) ŌĆó Nonrefractive Accommodative ET with or without high AC/A ŌĆó Intermittent esotropia ŌĆó Recognize risk factors ŌĆó Taper earlier than we were taught https://www.kindpng.com/picc/m/481-4819822_transparent-light- bulb-idea-clipart-take-home-message.png
- 17. Possible Risk Factors ŌĆóPoor follow-up ŌĆóWrong prescription ŌĆóHigh AC/A ŌĆóPrematurity ŌĆóRapid control of deviation ŌĆóRapid drop in refraction ŌĆóAmblyopia ŌĆóDVD ŌĆóIOOA ŌĆóRemote NPC
- 18. Management Pearls ŌĆó Full cycloplegic refraction ŌĆó 2 cycles good control: consider reduce plus 1-1.5D from full cycloplegic refraction ŌĆó Intermediate or Short acting cycloplegic refraction ŌĆó If ET controlled, No need to run after latent hyperopia if ET controlled with Rx ŌĆó Iff residual ET, proceed with atropine refraction ŌĆó Closer follow-up than we were used to data:image/jpeg
- 19. References 1. Santiago AP (2022). Spontaneous Consecutive Exotropia After Accommodative Esotropia. Acta Medica Philippina (Online) https://doi.org/10.47895/amp.vi0.4540. 2. Lembo A, Serafino M, Strologo MD, Saunders RA, Trivedi RH, Villani E, et al. Accommodative esotropia: the state of the art. Int Ophthalmol. 2019 Feb; 39(2):497-505. doi: 10.1007/s10792-018-0821-6. PMID: 29332227. 3. Raab E. Accommodative Esotropia. Difficult Esotropia Entities: Principles of Management. In Clinical Strabismus Management Principles and Technique. Rosenbaum AL, Santiago AP (editors), Philadephia, WB Saunders, 1999, pp 140-143. 4. Shin DH, Choi CY, Han SY. Risk factors for spontaneous consecutive exotropia in children with refractive and nonrefractive accommodative esotropia. Jpn J Ophthalmol. 2020 May; 64(3):292-7. doi: 10.1007/s10384-020-00724-5. PMID: 32108919. 5. Senior JD, Chandna A, O'Connor AR. Spontaneous consecutive exotropia in childhood. Strabismus. 2009 Jan-Mar; 17(1):33-6. doi: 10.1080/09273970802678818. PMID: 19301191.
- 20. References 6. Weir CR, Cleary M, Dutton GN. Spontaneous consecutive exotropia in children with motor fusion. Br J Ophthalmol. 2001 Feb; 85(2):242-3. doi: 10.1136/bjo.85.2.238e. PMID: 11225577; PMCID: PMC1723827. 7. Beneish R, Williams F, Polomeno RC, Little JM. Consecutive exotropia after correction of hyperopia. Can J Ophthalmol. 1981 Jan; 16(1):16-8. PMID: 7470983. 8. Watanabe-Numata K, Hayasaka S, Watanabe K, Hayasaka Y, Kadoi C. Changes in deviation following correction of hyperopia in children with fully refractive accommodative esotropia. Ophthalmologica. 2000 Sep-Oct; 214(5):309-11. doi: 10.1159/000027511. PMID: 10965242. 9. Yurdakul NS, Ugurlu S. Analysis of risk factors for consecutive exotropia and review of the literature. J Pediatr Ophthalmol Strabismus. 2013 Sep-Oct; 50(5):268-73. doi: 10.3928/01913913-20130430-01. Epub 2013 May 7. PMID: 23641958. 10. Ha SG, Suh YW, Kim SH. Esodeviation without correction for tapering hyperopia in refractive accommodative esotropia. Can J Ophthalmol. 2018 Oct; 53(5):453-7. doi: 10.1016/j.jcjo.2018.01.019. Epub 2018 Mar 16. PMID: 30340709.