






















Supracondylar fracture of the humerus
- 1. Dr. Santosh Batajoo Resident (Orthopedics)
- 2. ’é×Commonest fracture in children. Uncommon after the physes have closed. ’é×Also called MalgaigneŌĆÖs fracture. ’é×The humerus breaks just above the condyles.
- 3. ’é×The distal fragment may be displaced either posteriorly or anteriorly. ’é×Common in boys. ’é×Types- flexion & extension (90%).
- 5. ’é×Fall on the outstretched hand with forearm in pronation. ’é×The distal fragment is pushed backwards and twisted inwards.
- 6. ’é×Posterior angulations or displacement suggests a hyperextension injury (common). ’é×Anterior displacement is due to direct fall on the point of elbow with joint in flexion (rare).
- 7. ’é× Type I ŌĆō an undisplaced fracture. ’é× Type II ŌĆō an angulated fracture with posterior cortex still in continuity. IIA ŌĆō a less severe injury with the distal fragment merely angulated. IIB ŌĆō a severe injury; the fragment is both angulated and malrotated. ’é× Type III ŌĆō a completely displaced fracture.
- 9. ’é×History of fall. ’é×Pain in the elbow. ’é×Elbow is swollen and tender. ’é×S-deformity of the elbow (posterior). ’é×Bony landmarks are abnormal.
- 10. ’é×Both active and passive movements of the elbow are decreased. ’é×Assessment of the neurovascular status. ’é×Relationships between the tip of the olecranon and the epicondyle are normally aligned.
- 11. ’é×Posterior tilt and shift ’é×Proximal shift ’é×Medial tilt ’é×medial / lateral shift ’é×Internal rotation
- 12. X ŌĆō ray
- 13. ’é×seen clearly in lateral view. ’é×Fat pad sign in undisplaced fracture. ’é×Posteriorly displaced - fracture line runs obliquely downwards and forwards and distal fragment is tilted backwards or shifted backwards.
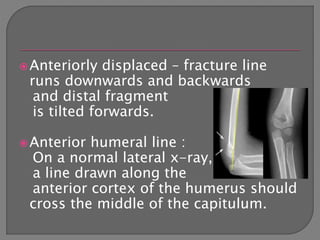
- 14. ’é×Anteriorly displaced ŌĆō fracture line runs downwards and backwards and distal fragment is tilted forwards. ’é×Anterior humeral line : On a normal lateral x-ray, a line drawn along the anterior cortex of the humerus should cross the middle of the capitulum.
- 15. ’é×Normal BaumannŌĆÖs angle is less than 80 degrees. ’é×Fish tail sign ’é×Crescent sign ’é×Coronoid line
- 17. UNDISPLACED ’é× The elbow is immobilized at 90 degrees and neutral rotation for 3 weeks. MILD POSTERIORLY ANGULATED ’é× Reduction under anaesthesia. ’é× If the reduction is unstable, the fracture should be fixed with percutaneous K- wires. ’é× Immobilized for 3 weeks
- 18. ANGULATED AND MALROTATED OR POSTERIORLY DISPLACED ’é×Usually associated with severe swelling, often unstable, risk of neurovascular injury. ’é×Reduced under general anaesthesia and then held with percutaneous K- wires.
- 20. ’é×Open reduction ŌĆō i. When fracture cannot be reduced closed; ii. An open fracture; iii. A fracture associated with vascular damage. iv. Interposition of the biceps
- 21. SKELETAL TRACTION with an olecranon pin i. Reduction cannot be achieved and manipulation is necessary. ii. Excessive swelling and circulatory compromise. iii. Inherently unstable fracture.
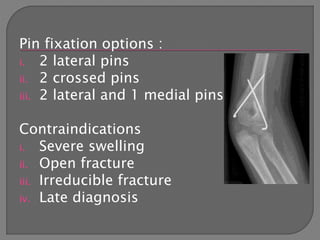
- 22. Pin fixation options : i. 2 lateral pins ii. 2 crossed pins iii. 2 lateral and 1 medial pins Contraindications i. Severe swelling ii. Open fracture iii. Irreducible fracture iv. Late diagnosis
- 23. FIXATION WITH PLATE AND SCREWS i. Cannot be reduced by closed measures ii. Wound is compound iii. Concurrent neurovascular injury iv. Concurrent forearm fracture v. If prolonged immobilization is to be avoided.
- 24. EARLY- ’é×Vascular injury- brachial artery ’é×Nerve injury- anterior interosseous n,>median n.>radial n.> ulnar n. ’é×VolkmanŌĆÖs ischemia & compartment syndrome
- 25. LATE- ’é×Malunion- uncorrected sideways tilt and rotation may lead to varus or valgus deformity. Gun stock deformity ’é×Elbow stiffness ’é×Myositis ossificans. ’é×Tardy ulnar nerve palsy ’é×Nonunion ŌĆō least common
- 27. Thank you..