Surgery for atrial fibrillation abhijit presentation
ŌĆó
0 likesŌĆó174 views

this presentation starts with the description of atrial fibrillation and goes on to describe the basis of it's surgical cure, viz. The Maze procedure. I then describe the technical aspects of Maze 1,2,3,4...





![AF maintaining substrate
ŌĆó AF begets AF
Structural remodeling (atrial
enlargement and ’¼übrosis, most
typically a’¼Ćecting the left atrium
[LA]), produces relatively ’¼üxed
reentry substrates
Progressive atrial dilation creates
longer conduction pathways for
reentry. Tissue ’¼übrosis slows
conduction, makes conduction
more heterogeneous, and creates
conduction barriers that favor re
entry](https://image.slidesharecdn.com/surgeryforatrialfibrillationabhijitpresentation-200214155407/85/Surgery-for-atrial-fibrillation-abhijit-presentation-6-320.jpg)







































Surgery for atrial fibrillation abhijit presentation
- 1. Surgery for Atrial Fibrillation Abh─│it Joshi NH
- 2. basic mechanisms ŌĆó concept of refractory period ŌĆó a faster source will eventually re-organise cardiac excitation ŌĆó what is re-entry? ŌĆó what are ectopic foci? what is macro and micro re-entry?
- 3. ŌĆó so now we know why: ŌĆó ectopic foci/’¼übrosis foci cause re-entry ŌĆó e’¼Ćect of chamber dilatation on macro re-entry
- 4. 3 atrial tachycardias ŌĆó focal ectopic tachycardia: no re-entry ŌĆó atrial ’¼éutter : single wavefront ŌĆó atrial ’¼übrillation : multiple (at least 2) wavefronts : multiple simultaneous irregular re entry circuits - unde’¼üned number of spatiotemporally varying wavelets and colli- sions
- 6. AF maintaining substrate ŌĆó AF begets AF Structural remodeling (atrial enlargement and ’¼übrosis, most typically a’¼Ćecting the left atrium [LA]), produces relatively ’¼üxed reentry substrates Progressive atrial dilation creates longer conduction pathways for reentry. Tissue ’¼übrosis slows conduction, makes conduction more heterogeneous, and creates conduction barriers that favor re entry
- 9. 3 problems in AF (1) palpitations, which cause the patient discomfort and anxiety; (2) loss of synchronous atrioventricular contraction, which compromises cardiac haemodynamics, resulting in varying degrees of ventricular dysfunction; and (3) stasis of blood ’¼éow thromboembolism and stroke contrast this with atrial ’¼éutter
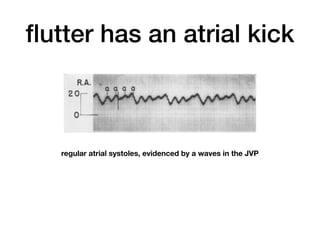
- 10. ’¼éutter has an atrial kick regular atrial systoles, evidenced by a waves in the JVP
- 11. remodelling in AF ŌĆó electrical remodelling : reduction in atrial e’¼Ćective refractory periods, increased spatial heterogeneity of refractoriness, and conduction slowing. ŌĆó structural remodelling : atrial dilatation, myocyte hypertrophy, sarcomere loss, glycogen accumulation, mitochondrial abnormalities, and the development of atrial ’¼übrosis. Atrial ’¼übrosis is thought to be a fundamental component of AF sustenance ŌĆó ’¼übrosis promotes AF and AF promotes Fibrosis : AF begets AF
- 13. hence AF needs.. ŌĆó a trigger : usually a premature depolarization or runs of focal ectopic depolarizations ŌĆó a macro re-entry circuit ŌĆó surgery for AF is directed at alteration of geometry and anatomy needed to support AF.
- 14. ŌĆó ŌĆ£ Fortunately, the macro-reentrant circuits that we had mapped in both dogs and patients were physically relatively large, that is, more than 5 to 6 cm in diameter in the left atrium and much larger than that in the right atrium. Therefore, atrial incisions placed no more than 5 to 6 cm apart should theoretically prevent the development of macro-reentrant circuits anywhere in the atria. It was clear that if macro-reentrant circuits could not develop in the atria, then the atria could not ’¼übrillate. The dilemma was how to place enough lesions on the atria┬Āto preclude the development of atrial macro-reentry (’¼übrillation) and leave behind an atrium that could be activated by the sinus node and still contract e’¼Ćectively.ŌĆØ - James Cox
- 15. if the atrium cannot develop macro re-entry circuits then it cannot ’¼übrillate, because thatŌĆÖs what a-’¼üb is by de’¼ünition.
- 16. initial surgeries ŌĆó 1980 : James Cox - left atrial isolation - ŌĆó electrical isolation of the LA, after recognition that most triggers are from the LA ŌĆó advantages : controlled the ventricular rate, alleviated palpitations, Right atrial kick was present and surprisingly increased LA preload because of this signi’¼ücantly improved haemodynamics ŌĆó drawback : LA still ’¼übrillated, thromboembolism risk continued ŌĆó eventually abandoned
- 17. ŌĆó Catheter Ablation of the Atrioventricular NodeŌĆōHis Bundle Complex. 1982 - Scheinman ŌĆó only alleviated palpitations and anxiety ŌĆó necessitated pacemaker ŌĆó no improvement in haemodynamics ŌĆó thromboembolism persists ŌĆó 1985, GiraudonŌĆÖs corridor procedure: isolated a strip of atrial septum harboring both the sinoatrial node and the atrioventricular node, thereby allowing the sinoatrial node to drive the ventricles. This procedure corrected the irregular heart beat associated with AF, but both atria either remained in ’¼übrillation or developed their own asynchronous intrinsic rhythm because they were isolated from the septal ŌĆ£corridor.ŌĆØ ŌĆó except for the requirement of a pacemaker, it su’¼Ćered all the drawbacks of ScheinmanŌĆÖs catheter ablation of the Bundle.
- 18. ŌĆó to cure AF, what was needed is to have lesions close enough to prevent macro re entry lesions to develop, at the same time maintain the pathway for conduction from SA node to AV node.
- 19. James Cox ŌĆ” That question was answered one Saturday afternoon while I was studying some of the BoineauŌĆōSchuessler experimental maps of atrial ’¼übrillation in my o’¼āce at Barnes Hospital. To better visualize the relationship between atrial anatomy and atrial electrophysiology, a rectangle was drawn to represent the entire mass of both atria 2-dimensionally.
- 20. ŌĆó ŌĆ£While studying this 2-dimensional representation of the atria with the superimposed electrophysiology of atrial ’¼übrillation, I suddenly realized that everything necessary to abolish atrial ’¼übrillation, while leaving the atrial activation and contraction intact afterward, could be accomplished by creating a pattern of lesions in the atria that was essentially that of a simple maze. The lesions could be placed close enough to prevent atrial macro-reentry, and if placed in a maze pattern, the SA node could serve as the site of entry of electrical activity into the atria and the AV node as its site of exit from the atria. One contiguous ŌĆ£true routeŌĆØ of conduction would be left intact between the entrance and exit sites, and multiple ŌĆ£blind alleysŌĆØ o’¼Ć this main conduction route would allow activation of all of the atrial myocardium, thereby preserving atrial contractility (Figure┬Ā1, D). One entrance, one exit, one true route between the two and multiple blind alleys ŌĆ” the pattern and principle of a maze.ŌĆØ
- 23. Maze 1 ŌĆó compromised the normal sinus tachycardia response ŌĆó LA conduction delayed ŌĆó both these : ŌĆ£chronotropic incompetenceŌĆØ ŌĆó high rate of pacemaker implantation
- 25. BachmannŌĆÖs bundle allows almost simultaneous activation of the 2 atria Maze 1 led to LA activation delay to the extent that LA was activated when the impulse had reached the LV
- 27. Maze 2 ŌĆó required SVC transection and was too di’¼ācult ŌĆó abandoned soon
- 29. Maze 3
- 30. Operation is performed via median sternotomy. Cannulae for venous uptake are placed in superior vena cava and through the low right atrium into inferior vena cava. Small venous cannulae (24F) and vacuum-assisted venous return are employed. Cardiopulmonary bypass is established, and tourniquets are tight- ened around venae cavae. First incision divides right atrial appendage and extends obliquely to midpoint of right atrial free wall. Medially, incision extends to atrioven- tricular groove. Longitudinal incision is made from superior to inferior vena cava along crista terminalis. Lower 2 cm of inci- sion is closed with a continuous suture of 4-0 polypropylene to prevent tearing during retraction. Vertical incision is made from point of closure to atrioventricular groove
- 31. Vertical incision is extended to tricuspid valve anulus in area of posterior lea’¼éet (2-oŌĆÖclock position, surgeonŌĆÖs view), working on endocardial surface of atrium cutting through the entire atrial wall. Residual myocardial ’¼übers are ablated by applying a 3-mm cryolesion (ŌłÆ70┬░C for 2 minutes) at tricuspid anulus. This portion of incision is closed with 4-0 polypropyl- ene suture.
- 32. Incision of medial aspect of right atrial appendage is continued into atrial groove to tricuspid valve anulus (10- oŌĆÖclock position, surgeonŌĆÖs view) by dis- secting on endocardial surface. A cryolesion is placed at anulus of tricuspid valve to ablate residual myocardial ’¼übers. This portion of incision is closed with 4-0 poly- propylene suture.
- 33. Aorta is occluded. Coronary sinus is cannulated, and cold cardioplegic solution is administered to achieve total electromechanical arrest. Left atrium is opened on right side behind interatrial groove and in front of pulmonary veins. Incision is extended superiorly and inferiorly. Atrial septum is divided at level of right superior pulmonary vein. This incision is curved inferiorly to divide the membrane of fossa ovalis.
- 34. Atrial septum is retracted anteriorly. Pulmonary vein encircling incision is developed, working within left atrium by extending incision across back wall of atrium above and below left pulmonary veins.
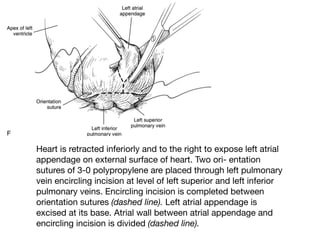
- 35. Heart is retracted inferiorly and to the right to expose left atrial appendage on external surface of heart. Two ori- entation sutures of 3-0 polypropylene are placed through left pulmonary vein encircling incision at level of left superior and left inferior pulmonary veins. Encircling incision is completed between orientation sutures (dashed line). Left atrial appendage is excised at its base. Atrial wall between atrial appendage and encircling incision is divided (dashed line).
- 36. Orientation sutures are tied, then used to close left atrium between them. Separate suture of 3-0 polypropylene is used to close bridge to and base of left atrial appendage.
- 37. Exposure returns to interior of left atrium. Orientation sutures are passed inside left atrium and used to close encircling incision superiorly to midpoint and inferiorly for about 2 cm of posterior wall of left atrium. Vertical incision is developed between encircling incision and mitral valve anulus. Incision is through entire left atrial wall into epicardial fat in atrioventricular groove, exposing coronary sinus. A cryolesion is made on exterior surface of coronary sinus, using a 15-mm cryoprobe applied for 3 minutes. After 1 minute, a 3-mm cryoprobe is placed on mitral valve anulus and a 2-minute cryolesion is made. Vertical incision is closed with 4-0 polypropylene. Mitral valve repair or
- 38. Pulmonary vein encircling incision is closed to pulmonary veins on right side. Retraction is switched to right atrium, allowing all but ’¼ünal centimeter of encircling incision to be closed. Left ventricular venting catheter is placed through separate incision in right superior pulmonary vein.
- 41. ONCE AGAIN !
- 42. Maze 4
- 44. Hassaiguerre et al - 1998, NEJM ŌĆó studied 45 patients with frequent episodes of atrial ’¼übrillation refractory to drug therapy. ŌĆó The spontaneous initiation of atrial ’¼übrillation was mapped with the use of multielectrode catheters ŌĆó Three foci were in the right atrium, 1 in the posterior left atrium, and 65 (94 percent) in the pulmonary veins (31 in the left superior, 17 in the right superior, 11 in the left inferior, and 6 in the right inferior pulmonary vein). ŌĆó laid down the basis for PVI
- 45. ŌĆó RA is the trigger source in 15% ŌĆó also, addressing only the RA, frequent post procedure ’¼éutter is there
- 47. Energy sources for ablation
- 49. Thank You